


Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS
Hi, it’s Patrik Hutzel from INTENSIVECAREHOTLINE.COM where we instantly improve the lives for Families of critically ill Patients in Intensive Care, so that you can make informed decisions, have PEACE OF MIND, real power, real control and so that you can influence decision making fast, even if you’re not a doctor or a nurse in Intensive Care!
This is another episode of “YOUR QUESTIONS ANSWERED“ and in last week’s episode I answered another question from our readers and the question was
My Mother Had a Cardiac Arrest and Her WBC is Increasing. Is It A Sign That She is Getting Worse?
You can check out last week’s question by clicking on the link here.
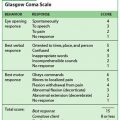
In this week’s episode of “YOUR QUESTIONS ANSWERED” I want to answer questions from one of my clients Stephanie as part of my 1:1 consulting and advocacy service! Stephanie’s mother is a post cardiac arrest patient in the ICU and Stephanie is asking if Glasgow Coma Scale (GCS) of 3 is a result of brain injury or the Phenobarbital.
My Mother Had a Cardiac Arrest and is Still in a Coma. Help!

Patrik: Yes, no I appreciate that. And there’s nothing standing in her way to have a trach? She’s not bleeding, her INR and her APTT are normal?
Eva: She does have some of the Cangrelor on, a blood thinner, she does have that running, but, she is not, there’s no more blood in the urine, there’s no sign of bleeding. Nothing like that, so, I don’t see why there wouldn’t be a reason to able to be trach and PEG. You know what I mean, like we would still do it, even if she was on Heparin or what have you. They would probably stop the Cangrelor before they do the procedure.
Patrik: Exactly, absolutely. Look, I really appreciate your time and your help. I’m sure you’re busy.
Eva: Absolutely, I’m glad we got a good line, because I couldn’t, I was like this is so frustrating, I couldn’t hear anything they were asking me.
Patrik: This is a very good line, look I really appreciate your help and your insights. Have a good shift, thank you so much!
Eva: You too, thank you take care.
Patrik: Bye-bye.
Eva: You still there Miranda? Miranda? Hey, you still there?
Recommended:
Miranda: Yes, ma’am.
Eva: Okay.
Miranda: I had wanted to know, at this present moment, I appreciate you for you’re-
Eva: No, absolutely, absolutely. No, I’m glad I got to talk to you. Like I said, I’ve kind of just kind of, this is my busy time, as you probably know, so it’s been kind of back and forth with patients, so.
Miranda: Okay, thank you again.
Eva: No, absolutely talk to you later, okay?
Patrik: Okay, everybody there?
Miranda: Can you hear me?
Patrik: I can hear you.
Rebecca: Yeah. Last night, the nurse draw some of blood, so I went up there and I got the chart, and I got a temperature has been elevated up to 44 degrees because they were trying to regulate it, but they have not been able to regulate it. I was there. Tonight, this is the first time it’s been regulated, because I’m there, and not only am I there, I’m watching, looking and I went and had Mikael taken off of my sister primary care because, he was incompetent, was playing music stuff over his ears, and also I was asking him to change his gloves because that’s why, I don’t know if he is incompetent or the other nurses are incompetent. I went to head nurse, and I know, when you are administering medicine to patients and between patients you know, you do not change gloves. It’s just things that are going on. Cause I been here for 6 days, and I don’t why it’s happening. My other sister she came up and I was like. That’s it. I’m on my way to the hospital.
George: I’ll walk you out.
Miranda: Mr. Patrik.
Patrik: Yes?
Miranda: The only thing that they keep saying is Phenobarbital is not affecting her.
Patrik: That’s what they’re saying. I understand it’s the lowest dose she can possibly be on. But she claims that Carmen hasn’t been on any sedation for the last seven days, I mean Phenobarbital is sedation. If you typed Phenobarbital into Google, you would find that it’s sedation. You know. Can you hear me, because I’ve got a really poor line?
Stephanie: That’s because of this piece of paper. Is this a little bit better?
Patrik: Oh, much better. Now, it’s interfering again.
Stephanie: Oh, wow it must be her house.
Patrik: That’s better now.
Stephanie: Okay, is this okay right here?
Patrik: Oh, much better.
Recommended:
Stephanie: Okay.
Patrik: So, even though she’s saying that Phenobarbital is not a sedative, from my experience it definitely is, and she may be on a low dose, but it’s hard to say at the moment whether the GCS three, like her not responding, is an effect of the brain injury or of the sedation. I mean the nurse says it’s the result of the brain injury. But I still argue it’s way too early.
Stephanie: It’s too early to do what?
Patrik: It’s way too early to determine, you know, can she wake up, or can’t she wake up? It sounds to me like they’ve got the seizures under control, now. Like, she hasn’t been having a seizure now for a few days. That’s good. But, because they’ve got the seizures under control, that means she’s getting a fair amount of anti-seizure medication.
And that can stop her from waking up, as well. And, sorry, just let me mention one more thing. And she’s got the Ativan as well. That’s all keeping her sedated to a degree. You know, so, the other thing that you may have heard me asking is, I think she will need a trach. I think there is no way around that. And, talking to the nurse, we all think she’s ready for that. That’s the logical next step.
The other thing that I haven’t mentioned in all of this, but probably one of the next steps, once she has a trach, she should be able to get mobilised and get out of bed, for example.
Stephanie: Right.
Patrik: And that would stimulate her. She needs gentle stimulation. Very gentle. Do you think she’s getting any stimulation at the moment?
Stephanie: No, nobody’s coming around rubbing her or anything. The bed, it’s an airbed or whatever it is that’s supposed to, what does the bed do, Miranda? Some kind of a pump in the bed, but that’s not enough. I don’t ever have a report you had on that, Patrik. That’s not enough. They were changing her from side, turning her from side to side. But I don’t know if they’re doing that or not. Rebecca would know that.
They still turn her side to side. As well as the bed pump, like an airbed kind of thing.
Patrik: Well, they would turn her a few times a day, but that’s basic nursing care, that’s not stimulation, really. That’s basic nursing care.
Recommended:
Stephanie: Not like every two hours, you know what I mean?
Patrik: Yeah, they should do it every two hours, every two to three hours. But what I’m staying, once she has the trach, it would be much safer to get her out of bed.
Stephanie: Right, and the sooner she can sit up.
Patrik: Correct. Because that’s going to be critical to find out if she’s responding to that or not. Because literally, she has been lying flat for the last two weeks.
Stephanie: Exactly. Okay, so,
Patrik: So, given that, and this is the other thing, she’s not, you know, you might remember last week when we spoke, I mentioned that goal was always to get somebody off the ventilator and the breathing tube. Now that I have more insight from the nurse, she’s still getting most of the breathing from the ventilator which means she’s not ready to have that breathing tube removed, which means, a tracheostomy at this point is inevitable.
Stephanie: Yeah, okay. You mean, she’s not ready to go without any ventilation at all.
Patrik: No. That’s right. That’s exactly right. Which is why I asked, where is she at in terms of like can she breathe by herself? And she said, well, she’s taking a few breaths, but the majority of the work is still coming from the ventilator.
Stephanie: Did she give you a number?
Patrik: Yes. 16 breaths per minute, from the ventilator. Plus a few breaths she’s taking by herself. But not enough to sustain spontaneous ventilation.
Stephanie: Okay. So then, tomorrow, any questions right now? Anybody? So then tomorrow, when we have the meeting at 11 o’clock, what are we going to say to the neurologist who’s meeting with us?
Patrik: Yeah, that’s a good point. So, did you hear me asking, I asked the nurse, did she think that since you’re not waking up, it’s the brain injury or is it the sedation?
Stephanie: Hold on one second.
Patrik: Sure.
Recommended:
Stephanie: Okay, go right ahead.
Patrik: So, tomorrow, we need to ask, you remember? I asked the nurse a moment ago, whether she thinks, since she’s not waking up, it’s a result of the brain injury or a result of the sedation. She thinks it’s a result probably of the brain injury. And that’s the question we need to pose to the neurologist tomorrow. But then, at the same time, let me ask you, have you seen a report of the CT Scan? Have you seen that?
Stephanie: We’ve seen no reports.
Patrik: Right, you haven’t seen it have you? Okay, if I was you, I would try and get that report before the meeting tomorrow.
Stephanie: Yeah, I would try, because there could be something in the report that could be quite important.
Yeah, probably to send a picture in WhatsApp or via email. So, right.
Patrik: Just ask them. Yes, so, and then, another question, for example is, what are the next steps? Once you have the trach, what are the neurologist predict as the next step? For example, would she think that she can she go to neuro rehab? Is that a question that has been asked along the way?
Stephanie: Neuro rehab, but no talk about neural rehab? And other questions that are important is how are they going to manage the seizures going forward? I mean, she hasn’t had seizures. Okay, so the critical point is really, well, she’s seizure-free at the moment, that’s all good. Okay, but, they need to reduce some of the seizure medication to give her a chance to wake up.
Patrik: Well, they need to try. They need to find the right level. The right level of seizure medication to keep her seizure-free, but also, to give her a chance to wake up. I mean, their first goal was to stop the seizures. That was their first goal. They achieved that by giving her more than she needs.
Stephanie: Now, because I understand that in the beginning her seizures were quite severe, right? So, now is time, now that she’s seizure-free, now is the time to minimise seizure medication, and see, can they wake her up by minimising seizure medication.
Recommended:
Yeah. Right, I see, when I asked the nurse a moment ago, she didn’t mention any of that. I didn’t specifically ask that, I just asked the seizure then she said, well, I haven’t seen a seizure. And again, we probably need to ask that tomorrow whether does she have seizures or neuro storm, we need to clarify that.
Patrik: Pardon? Right. So, those are the questions. Has the neurologist given an opinion about the trach? Have they commented on the trach, what they think about the trach?
Stephanie: Yeah, that’s fine. I’m all for it. That’s all fine.
Patrik: Can’t hear that, can you say that again please, Miranda?
Right. Okay, no I understand. And this is again where I say, number one, making her comfortable could be euthanasia that’s number one. Number two, a trach will buy Carmen all the time she needs. Okay, so at the moment, you would’ve heard the nurse saying, you know, the tongue is swollen, and nobody should have a breathing tube for longer than two weeks, and I agree with all of that. Right? But a tracheostomy really will buy Carmen time to wake up. Right? How long does this take? Nobody knows.
Stephanie: But it will give her the opportunity to wake up.
Patrik: That’s exactly right, and that’s what I said to you yesterday, Stephanie and Miranda. That, nobody in intensive care know what quality of life looks like down the line. Nobody has a crystal ball. And also, if for whatever reason, like we talked about yesterday, she’s not getting better, you can still talk about end of life. There’s no hurry. It takes time, you know?
Stephanie: Yep, yep.
Yes, I can, and I did hear what the doctor said, I did hear. I think a central line is fine. I think it’s a sign that there is an infection, because her blood pressure is dropping. It’s also a sign to me that she’s nowhere ready to go to LTAC, because that’s critical care, what they’re doing. That’s intensive care treatment. Right, a central line. And now they will be starting her on some vasopressors. That is intensive care treatment, which is another sign she is nowhere ready to go to LTAC. But a central line, from what she describes, is the next logical step.
Recommended:
Yes, they can, one goes with the other. They can’t really do one without the other.
Stephanie: Something about side effects, but I didn’t, she’s just probably referring to complication. Right. Yeah, they would put in the central line first, because that’s first before the A-line. But, you see what I’m saying is, with the central line, and then they start her on vasopressors, right? And then she will need an A-line to monitor her blood pressure. So, it’s unfortunately to have, one with the other.
Yeah, you see, that, to me is a sign that she’s getting infection, and that’s a shame. This is also why I’ve been so vocal about that she’s not going to LTAC because these things do happen, and when they do happen, you want her to be in the right environment.
Patrik: Yeah, I wouldn’t be too worried about it at this stage. And like I said to you last night, as well as now, we’re not over-complicating. We’re talking to the right people, you know? That’s all you need to know, let’s take one step at the time. But they can’t force you to go to LTAC. They can’t force you.
Stephanie: Say that again, please?
Patrik: I would no. That’s, again, what does a rumour mean? I tell you, as long as the insurance is not going to call you and say, hey, you’re running out of entitlements, you know, this is a life or death situation. I mean, very rarely have I seen that the insurance is not paying. If they don’t pay, there’s a process.
Stephanie: Yeah. That would be new to me. I think another, I would not worry about that at this stage. I mean, this is life or death. Life or death is often not about who’s paying.
Patrik: Yes, I’m listening, I’ve listened to all of this. So, what they are suggesting makes sense, right? It all makes sense in terms of giving her the blood product first, if that doesn’t work, put in the central line and then give some inotropes, it all makes sense to me I don’t see anything wrong in what they’re doing. And it’s also sign to me, it really is a sign to me, that if she was to go to LTAC they wouldn’t be able to manage those emergency situations like they do now. Here, in ICU, they have the skills to manage that.
Blindsided by… Right. But it sounds like it’s a new thing, it only happened in the last 24 hours. Oh, I see, I see. Because they know somebody’s asking questions. Right, sure.
For sure. By the same token, if she does drop her blood pressure, they have to do something. Because that’s what it sounds like has happened also. She’s dropping her blood pressure.
Recommended:
Yeah, she did. Yeah, so bear in mind, this is all coming back again to issues like, what I kept saying in the last few days, she’s not ready for LTAC. Because the last thing she needs at the moment in such a vulnerable state, is to go somewhere else. That’s the last thing she needs. She’s too vulnerable. You know, absolutely.
Patrik: Say that again? Look, at the moment from what I can see, they’re doing everything they can. From what I can see. Right. But, my concern is clearly that if she wants to go into LTAC that she wouldn’t get what she needs. Right? That would be my concern. But at the moment, I have no concern in what they’re doing now, with what they’ve shared. I have no concern.
Stephanie: Yeah, I think trach is fine. I have no, I really have no- I think the trach needs to happen, especially in light of an infection potentially, right? I think a trach is inevitable. But, you see the other thing, the discussions tomorrow could potentially be about LTAC, it could be about rehab, it could be about end of life, but if, if you were interested in potentially end of life, you would have to stop them from doing what they’re doing.
Patrik: Because now they’re escalating treatment because Carmen is deteriorating, slowly. So, now they literally asked you now, are you okay with escalating treatment?
No, no, intubate. No, no, at the moment, she’s intubated. The breathing tube is intubation. If you extubate, without the trach, it’s a very high change she will die. Yeah. Look, you see, with the PEG, what does she have at the moment? Does she have a nasogastric tube? Does she have a feeding tube through her nose? You could leave that for a while, but while they’re doing the trach, you might as well do the PEG. It’s up to you. Right, that’s fine. You got to be way up, a trach and a PEG will buy Carmen time to wake up. We don’t know whether she’s going to do that or not, but it will buy her the time to wake up.
Recommended:
That’s the goal, and if for whatever reason, Carmen is not improving, there’s still plenty of time to talk about end of life. You know what I mean? That’s exactly right. Very much so.
Okay, please let me know tomorrow, 11:00, is it? Yeah, I’ll be there. We can quickly talk beforehand if you like, or if you need anything in the meantime, please let me know.
Patrik: The CT scan report. I also, just a moment ago, I put a link into WhatsApp about Phenobarbital. You can have a look there. Okay. Please let me know what you need next before the meeting, or if you have any other questions before the meeting, please let me know and we’ll talk. Okay, you’re very welcome, all the best. Bye!
The 1:1 consulting session will continue in next week’s episode.
How can you become the best advocate for your critically ill loved one, make informed decisions, get peace of mind, control, power and influence quickly, whilst your loved one is critically ill in Intensive Care?
You get to that all important feeling of making informed decisions, get PEACE OF MIND, CONTROL, POWER AND INFLUENCE when you download your FREE “INSTANT IMPACT” report NOW by entering your email below!
In Your FREE “INSTANT IMPACT” report you’ll learn quickly how to make informed decisions, get PEACE OF MIND, real power and real control and how you can influence decision making fast, whilst your loved one is critically ill in Intensive Care! Your FREE “INSTANT IMPACT” Report gives you in-depth insight that you must know whilst your loved one is critically ill or is even dying in Intensive Care!
Sign up and download your FREE “INSTANT IMPACT” REPORT now by entering your email below! In your FREE “INSTANT IMPACT” REPORT you’ll learn how to speak the “secret” Intensive Care language so that the doctors and the nurses know straight away that you are an insider and that you know and understand what’s really happening in Intensive Care! In your FREE report you’ll also discover
- How to ask the doctors and the nurses the right questions
- Discover the many competing interests in Intensive Care and how your critically ill loved one’s treatment may depend on those competing interests
- How to eliminate fear, frustration, stress, struggle and vulnerability even if your loved one is dying
- 5 mind blowing tips & strategies helping you to get on the right path to making informed decisions, get PEACE OF MIND, control, power and influence in your situation
- You’ll get real world examples that you can easily adapt to your and your critically ill loved one’s situation
- How to stop being intimidated by the Intensive Care team and how you will be seen as equals
- You’ll get crucial ‘behind the scenes’ insight so that you know and understand what is really happening in Intensive Care
- How you need to manage doctors and nurses in Intensive Care (it’s not what you think)
Thank you for tuning into this week’s YOUR QUESTIONS ANSWERED episode and I’ll see you again in another update next week!
Make sure you also check out our “blog” section for more tips and strategies or send me an email to [email protected] with your questions!
Also, have a look at our membership site INTENSIVECARESUPPORT.ORG for families of critically ill Patients in Intensive Care here.
Or you can call us! Find phone numbers on our contact tab.
Also check out our Ebook section where you get more Ebooks, Videos and Audio recordings and where you can also get 1:1 counselling/consulting with me via Skype, over the phone or via email by clicking on the products tab!
This is Patrik Hutzel from INTENSIVECAREHOTLINE.COM and I’ll see you again next week with another update!
Related Articles:
- 5 Ways to have control, power and influence while your loved one is critically ill in Intensive Care
Related Articles:
 My Wife Has Been Declared Brain-Dead in the ICU. Why are They in a Hurry to Withdraw Treatment to Her?
My Wife Has Been Declared Brain-Dead in the ICU. Why are They in a Hurry to Withdraw Treatment to Her?
 My Tracheostomized Husband was in ICU, now in LTACH. What are the Priorities for His Recovery?
My Tracheostomized Husband was in ICU, now in LTACH. What are the Priorities for His Recovery?
 My Critically Ill Husband is On Dialysis and in ICU due to Septic Shock. Which organ is more important, the Heart or the Kidneys?
My Critically Ill Husband is On Dialysis and in ICU due to Septic Shock. Which organ is more important, the Heart or the Kidneys?
 My Mother is in the ICU after Cardiac Arrest. How Soon Will She Be Oriented and Extubated?
My Mother is in the ICU after Cardiac Arrest. How Soon Will She Be Oriented and Extubated?
 My Mother Had a Cardiac Arrest and Her GCS is 3. Will She Be Weaned from the Ventilator?
My Mother Had a Cardiac Arrest and Her GCS is 3. Will She Be Weaned from the Ventilator?