


Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS
Hi, it’s Patrik Hutzel from INTENSIVECAREHOTLINE.COM where we instantly improve the lives for Families of critically ill Patients in Intensive Care, so that you can make informed decisions, have PEACE OF MIND, real power, real control and so that you can influence decision making fast, even if you’re not a doctor or a nurse in Intensive Care!
This is another episode of “YOUR QUESTIONS ANSWERED” and in last week’s episode I answered another question from our readers and the question was
You can check out last week’s question by clicking on the link here.
In this week’s episode of “YOUR QUESTIONS ANSWERED” I want to answer questions from one of my clients Stephanie as part of my 1:1 consulting and advocacy service! Stephanie’s mother is a post cardiac arrest patient in the ICU and Stephanie is asking why the ICU team thinks that as long as her mom is in the ICU on life support, they always have the option to stop treatment.
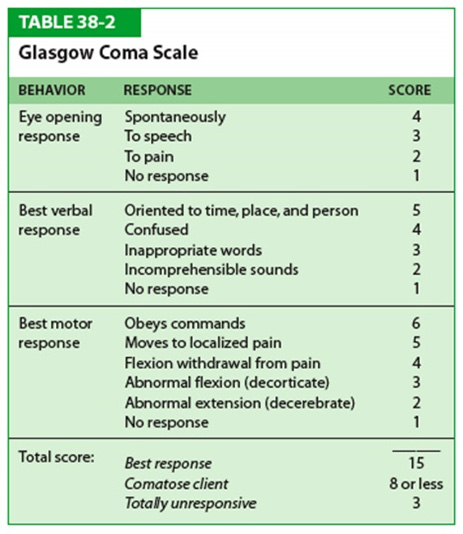
My Mother Had a Cardiac Arrest and Her GCS is 3. Will She Be Weaned from the Ventilator?
Stephanie: Right, they say she’s got five and she’s got abnormal activity and I did question the fact that Phenobarbital is a sedative, but they said it’s not enough to do blah, blah, blah, and I said “Well, what else is she on, what else is she on?” They said … I said “Is she on Keppra?” Now he said “She’s on …” oh, what’s the other one?
Patrik: Keppra, Dilantin?
Stephanie: No, Vi … Vim-
Patrik: Vimpat?
Stephanie: Vimpat I think.
Patrik: Okay-
Stephanie: That’s not a sedative, right?
Patrik: It’s not a sedative, it’s an anti-seizure medication.
Stephanie: Right, exactly.
Patrik: What about-
Stephanie: Hold on, hold on, they said Vimpat is the same as Depakote?
Patrik: Yeah, it is, it is.
Recommended:
Stephanie: Okay, good, that’s what they said she’s on.
Patrik: And, who was in the meeting again? Who was in the meeting? Was it Dr. Reynolds and the neurologist? Who was there?
Stephanie: Yes, exactly, there was only those two.
Patrik: Dr. Reynolds and the neurologist.
Stephanie: Oh hold on, and the social worker. We didn’t have all of our, and there was only one, two, three, four of us. There’s Livy there was myself, there was Tonette and there was Miranda. But my brother wasn’t there or my older sister was not there.
Patrik: Right. And, did you feel like, I mean last week when you first contacted me you felt like you were under a lot of pressure. Did you feel yesterday that the pressure was less?
Stephanie: Yes, I did. Today, today, today-
Patrik: Yeah, yeah, of course.
Stephanie: So, today is for here is, today is Monday.
Patrik: Monday, yeah, yeah, for me too but in morning.
Stephanie: Yep, this morning, sure.
Patrik: That’s all right, that’s all right. So, you felt like the pressure has eased already?
Stephanie: Oh, yeah, and I think more I go on the ward, he says “I work for you, can you tell me what to do?” I say “Well, this is how we feel about it, you know. You talk about quality of life, you don’t even know what her quality of life is going to be. How do you know what her quality of life is until we’ve given her a chance?” You know, he said “Well, she’s been off her seizure medicine for a week and she hasn’t woken up”. I said “Well, these things take time”. You know, you think she hasn’t woke up, I said “She’s still on the medication”. He said “We can’t take her off” or whatever because of the seizures and whatever.
Patrik: And that’s going to be a fine line between getting her to wake up, it’s going to be a very fine line between getting her to wake up and not having seizures. That’s going to be a very fine line. Any more talk about end of life? Any more talk about that?
Stephanie: Yeah but it didn’t sort of stop until we tell them that’s not what we interested in.
Patrik: Right, right, so they-
Stephanie: Yeah, we told them that all we wanted was to keep … you know, I kind of got something in right away. I think Miranda got up and said something and he said “Well yeah, you know, what do you want?” I said “Well, it’s not complicated” I said “We understand, we’re not oblivious to what the options are” I said “But, what we’re interested in is getting Carmen to this was raised and we just want her to have the trach and the stomach tube and the arterial thing”, we agreed to all three of those, you know, you get her stable and yeah, at this point we’re not thinking about making her comfortable. To say that what, how comfortable her life is, we don’t know, she isn’t … as far as we’re concerned, she hasn’t had time to think or to wake up, from her medicine or whatever. You may feel that she has, but I feel like she has a fighting chance, you know.
And, we don’t know that until we do. I said “And, of course if we do the trach and we give her a chance to become stable, and down the line we decide that okay, this is not working, we can make the decision at that time”.
Recommended:
Patrik: Correct.
Stephanie: But we cannot make that decision without giving Carmen a chance. My sister Miranda told me Carmen was blinking her eyes today.
Patrik: Right, right … and you see this is so often what happens, you know. I can’t stress enough that people in a situation like that need time. Right, I can’t stress that enough. Now, do people have time? They really don’t because every day in an induced coma, or in a coma, there’s muscle wastage, you know weaken people…
Stephanie: That’s right, deterioration. They say she has deteriorated over the weekend.
Patrik: Correct.
Stephanie: Well I guess she has, you know.
Patrik: But she’s alive.
Stephanie: You know, we can’t really work a trace off her we can’t even get her online now because I said “I’m not talking about them taking the trach out, I mean taking the intubate and the tube out, I’m talking about switching over to the trach”.
Patrik: That’s right, you know and she is you know … for example, when we work with clients sometimes who have been in ICU long term, you know there is this whole issue of muscle wastage and they need to basically learn to mobilise again, learn to walk again, you know. It’s not easy, you know, but withdrawing treatment, you know, people are dead. Then it’s all too late.
Stephanie: Well let me tell you, Miranda said to them, you know, “I’m just believing”. She said “We are a believing family”. And, he was “I have never seen the love. She must be a much loved person. You guys have been here just about 24/7. I have seen no other family up here as much as I’ve seen your family here you know with your loved one and concerned about her care”. And, Miranda said, you know, she says “I, as far the quality of life”, she started related stories to them about people that she know who you guys said were probably dead, you know, and they came back and they be walking and they’re talking, you know. I would like nothing, even if I’m likely to come back 1 or 2%, I would like nothing more than for my mother to look at me in my face and smile and you know, and give me some emotions and this that and the other. She said “You know, my grandmother, you know really didn’t want her to stay in hospital, wanted to make my mother comfortable” but I said “I’m sorry, I don’t think she’s at that stage”.
Recommended:
She may not be able to talk, and yes she did have a stroke that affected her, I think her frontal lobe or whatever, so that she couldn’t speak and so I said, we just went before the ethics committee and said “You talking about a woman who you come down the hall, and you come in here, she smiles at you, she starts shaking her shawl looks like she’s dancing, you know, takes your hand and put it up against her face and kiss your hand. I’m sorry, I don’t think she ready to go. I think she has some personality, she just not able to verbalise, you know and she is having other issues but I don’t think she’s end stage. I mean, I’m sorry, everybody’s end stage you want to get to that point, eventually we going to die, okay”.
Patrik: We accept that.
Stephanie: Yeah.
Patrik: You know we-
Stephanie: Well we accept that, but at this point we’re not ready to pull those leads. Like you said, euthanasia.
Patrik: That’s right and as long as she’s in ICU on life support, you know, the option to stop is always there.
Stephanie: There’s nothing.
Patrik: The option to stop is always there. There is no hurry.
Stephanie: Right, right.
Patrik: So, but it’s good, you know you can see that we’re starting to ask the right questions and with not giving into their pressure, you can see the dynamics are changing. Would you agree with that, that the dynamics are slightly changing, or?
Recommended:
Stephanie: Yes, yes I would, yes, I would, I would, I would say that because we’re all, look here we’re all, we’re excited about little Milton. We want to meet him. Talking to them as a family and he was chit-chatting and talking and discussing and we were saying how that it was funny how that if he says we don’t believe anything they say because one minute they say this and the next minute they say that, you know. Now, all of a sudden, they’re trying to take care of her, you know, but that’s because I think they were just trying to … and really wasn’t … when they saw that fluid immediately they should address that.
Patrik: Absolutely, and I’m sure they will.
Stephanie: No, they’re addressing it today. I’m sure they’re addressing it. I’m not there, but I’m sure they’re addressing it today. It was obvious that they are because number one, before we left this afternoon, they were testing to see where she was. You know, and I said “What can you do to mitigate that?” Because, so we couldn’t use blankets so we … I don’t know exactly what Arnold said he’s doing so I need to … that’s a question I need to write down, what are you doing to actually mitigate … you found how much fluid it is, what are you going to do? Now you said her blood pressure is high, kind like well somebody said well maybe 80, that was her mean, you know, something like that but, so that’s not a bad mean, but it’s probably a little higher than what they want it to be, but they don’t want it lower than 68 or something like that.
Patrik: Yep, yep, yep.
Stephanie: Does that sound right Patrik?
Patrik: It does and I’ll tell you why it sounds right. The cut off for a mean blood pressure is sort of 60 to 65, why? Because the kidneys … if the mean blood pressure is less than 60 or 65, the kidneys don’t get enough perfusion.
Stephanie: Okay, what if it’s 88?
Patrik: Yeah, that was the upper one. You mentioned earlier the mean was around 60 to 65.
Stephanie: Well, no, no, no, that’s what he said it had been that but it’s come up, if I’m not mistaken.
Patrik: Okay, so are you saying the mean blood pressure is 98?
Recommended:
Stephanie: That’s what I think is the last thing he told me today. So, he said-
Patrik: That would be high.
Stephanie: High. But being that way he said we don’t need the arterial line.
Patrik: Right, okay.
Stephanie: We need to make a phone call, we need to make a phone call.
Patrik: No, no, we need to make a phone call but with what you are sharing I argue they don’t need the arterial line and I’ll tell you why-
Stephanie: But, Dr Abdul said we don’t need it.
Patrik: But, yeah and I tell you why he could be right because, you remember yesterday, they were talking about the blood pressure being low. Do you remember that?
Stephanie: Mm-hmm (affirmative), yes.
Patrik: And they were talking about putting a central line in and giving vasopressors because of the low blood pressure. Then they said they would give her a blood transfusion first and if she responds to the blood transfusion, they wouldn’t need the central line and they wouldn’t need the vasopressors. Do you remember that?
Stephanie: Yes, but I don’t think they even needed that. I don’t think they gave her any blood either.
Patrik: Right, okay, okay, okay, fine, fine. But with the blood pressure coming up they wouldn’t need any vasopressors which would eliminate the need for the central line. I dispute not needing an arterial line. I really dispute that because as long as somebody’s on a ventilator and you want to wean them off the ventilator, the only problem is, the only way you can measure the effectiveness of a ventilator is with an arterial blood gas, right. I, to a degree, I dispute why no arterial line. So, then why has the blood pressure corrected itself? Maybe she’s correcting her infection already.
Stephanie: Yeah, I think so.
Recommended:
Patrik: Right, so that could be one of the reasons. If they started the antibiotics and they’re working, you know, infection is sort of correcting itself and blood pressure is coming up. Or, here’s another reason why blood pressure may go up, you know, I keep coming to that they need to minimise sedation and it sounds to me like all she’s on is the Phenobarbital and the Ativan at the moment, plus the anti-seizure, I really hope they are getting rid of that Phenobarbital as well as the Ativan, and if they do her blood pressure might come up as well.
Stephanie: Miranda saying “Well look if you don’t like this nurse, it obviously”. I don’t like the nurse that said that. I think she was the one from last night. They asked me to wait for rounds is the other issue, the antibiotics’ problem. I’m so hungry. I’ve got this salad when I leave here that you may not like as much. Okay, you want me to ask does she mind getting on the phone with you and me.
Patrik: Yes, please.
Stephanie: Okay, sure, you’re welcome. Can’t get anyone. She’s also at our meeting today. I’m feeling so overwhelmed seriously. I can’t come up here tomorrow at all at this stage. I hope our Livy can take it. Me and Livy went out today and had a little lunch and so she said she’s feeling, you know, so we had a chance to get away and just get a breather, you know what I mean.
Patrik: Mm-hmm (affirmative)
Stephanie: So we should, so hopefully that’ll help some. Oh, and I told you that they said that her coma scale was five.
Patrik: Mm-hmm (affirmative)
Recommended:
Stephanie: Well that’s good. That’s sort of moving in the right direction.
Patrik: Yeah, look it is. It’s better than three, but it’s not right. If it was up to an eight, I would say, now we’re seeing a little bit of light at the end of the tunnel.
Stephanie: Right, right.
Patrik: It’s still low. You know, so, yeah it’s better than three, but five is still incredibly concerning.
Stephanie: That’s why she needs to be off the sedative to see what happens. She seems really relaxed.
Patrik: Correct.
Stephanie: Well, now that we’ve been noticing.
Patrik: You know she.. Oh no go on, go on.
Stephanie: No, no, no it’s just that she seems relaxed and that she, you know she still has breath.
Patrik: It’s good that she looks relaxed because would you say a week ago she didn’t look relaxed?
Stephanie: I would say that she does not look as relaxed as she does now.
Patrik: Right. You know the Ativan for example would make her very relaxed. Would make her very relaxed. It depends how much she’s getting, but even the Phenobarbital would make her relaxed. I still, look and that could be something that I haven’t seen, even though I’ve seen a lot, I don’t think I’ve seen Phenobarbital being used in a situation like that. I just haven’t, which is, you know they’re telling you it’s the lowest dose she can be on, and that’s fine. I still feel like they need to stop it to see what she’s doing. But, is she coughing? Have you seen her coughing?
Stephanie: I don’t know. Let me ask Miranda. She asked me, was I on the phone with you now. I’m in here with my mother on phone with him. Were you able tell him when I get a little better I’m going to help you out so you haven’t asked, oh, what’s she talking about. We’re sitting here listening to music. Want to listen to music stimulating her brain and she has to find music she likes, okay. Can we call, I’m asking, can we call you? We call you for a minute. She’s avoiding the question in case you’ve noticed. She’s avoiding it I know because … yeah, it’s never easy. So it’s something I have to resign.
Recommended:
- YOU DON’T KNOW WHAT YOU DON’T KNOW WHEN YOUR LOVED ONE IS CRITICALLY ILL IN INTENSIVE CARE! (PART 1)
- YOU DON’T KNOW WHAT YOU DON’T KNOW WHEN YOUR LOVED ONE IS CRITICALLY ILL IN INTENSIVE CARE! (PART 2)
And then when you’re in the meeting there’s so many things that happen that you know, there’s just so many things. Everybody’s supposed to be taking notes but, you know, it’s not always easy. I got to find out where I put my notes. Okay, I know where they are. Okay, they made me fill out these forms.
I been trying to equip the family as much as I can. I gave them a copy of what you sent me, you know for the meeting, one, two, three, four, five, you know. We didn’t even get to discuss any of that because we just didn’t discuss it. It didn’t come up, you know, the one, two, three, four, five that you gave us, not yet. There was one thought that I think is that we shouldn’t … I try to tell myself don’t sign anything. I don’t want to beat up about this tonight because that will make them more anxious, you know what I mean?
Patrik: Mm-hmm (affirmative)
Stephanie: So, you think I should not mention it today, or do you think that it’s important that we try to withdraw that signature tomorrow, then we’ll do that.
Patrik: Yeah, I think … I mean I would not … in a situation like that, you already know they’re putting pressure on you.
Stephanie: Yeah.
Patrik: I would not –
Stephanie: Make a big deal of it.
Recommended:
Patrik: No, no, I would just probably remove it but also maybe send it to me. Maybe send it to me, you know and then I can have a quick look.
Stephanie: Yep, that makes sense that makes sense. Makes a lot of sense. Let me see what this says, oh … she says okay, she says okay, she’s okay, she says okay.
Patrik: Okay, so what do you mean okay? Do you want me to dial her in?
Stephanie: Yes, yes, yes, yes.
Patrik: Okay, so just give me one sec, I’ll dial her in, just give me one sec.
The 1:1 consulting session will continue in next week’s episode.
How can you become the best advocate for your critically ill loved one, make informed decisions, get peace of mind, control, power and influence quickly, whilst your loved one is critically ill in Intensive Care?
You get to that all important feeling of making informed decisions, get PEACE OF MIND, CONTROL, POWER AND INFLUENCE when you download your FREE “INSTANT IMPACT” report NOW by entering your email below!
In Your FREE “INSTANT IMPACT” report you’ll learn quickly how to make informed decisions, get PEACE OF MIND, real power and real control and how you can influence decision making fast, whilst your loved one is critically ill in Intensive Care! Your FREE “INSTANT IMPACT” Report gives you in-depth insight that you must know whilst your loved one is critically ill or is even dying in Intensive Care!
Sign up and download your FREE “INSTANT IMPACT” REPORT now by entering your email below! In your FREE “INSTANT IMPACT” REPORT you’ll learn how to speak the “secret” Intensive Care language so that the doctors and the nurses know straight away that you are an insider and that you know and understand what’s really happening in Intensive Care! In your FREE report you’ll also discover
- How to ask the doctors and the nurses the right questions
- Discover the many competing interests in Intensive Care and how your critically ill loved one’s treatment may depend on those competing interests
- How to eliminate fear, frustration, stress, struggle and vulnerability even if your loved one is dying
- 5 mind blowing tips & strategies helping you to get on the right path to making informed decisions, get PEACE OF MIND, control, power and influence in your situation
- You’ll get real world examples that you can easily adapt to your and your critically ill loved one’s situation
- How to stop being intimidated by the Intensive Care team and how you will be seen as equals
- You’ll get crucial ‘behind the scenes’ insight so that you know and understand what is really happening in Intensive Care
- How you need to manage doctors and nurses in Intensive Care (it’s not what you think)
Thank you for tuning into this week’s YOUR QUESTIONS ANSWERED episode and I’ll see you again in another update next week!
Make sure you also check out our “blog” section for more tips and strategies or send me an email to [email protected] with your questions!
Also, have a look at our membership site INTENSIVECARESUPPORT.ORG for families of critically ill Patients in Intensive Care here.
Or you can call us! Find phone numbers on our contact tab.
Also check out our Ebook section where you get more Ebooks, Videos and Audio recordings and where you can also get 1:1 counselling/consulting with me via Skype, over the phone or via email by clicking on the products tab!
This is Patrik Hutzel from INTENSIVECAREHOTLINE.COM and I’ll see you again next week with another update!
Related Articles:
- 5 Ways to have control, power and influence while your loved one is critically ill in Intensive Care
Related Articles:
 The ICU team is telling me and my mom to stop her medical treatment. Can they end her life without my consent?
The ICU team is telling me and my mom to stop her medical treatment. Can they end her life without my consent?
 The ICU Team Just Wanted to Empty Their Beds and Get Rid of My Dad. Is this Medical Malpractice?
The ICU Team Just Wanted to Empty Their Beds and Get Rid of My Dad. Is this Medical Malpractice?
 My Brother has COPD and Went into Cardiac Arrest. Does he Need to have an Immediate Lung Transplant because of Minimal Lung Function?
My Brother has COPD and Went into Cardiac Arrest. Does he Need to have an Immediate Lung Transplant because of Minimal Lung Function?
 My Mother is in the ICU for Post- Cardiac Arrest Care. Why Is She Having Seizures and isn’t Waking Up. I’m Tired of This Situation. Help!
My Mother is in the ICU for Post- Cardiac Arrest Care. Why Is She Having Seizures and isn’t Waking Up. I’m Tired of This Situation. Help!
 My Mom is in the ICU for Septic Shock. Why Do the ICU Team Wants Her To Be Discharged?
My Mom is in the ICU for Septic Shock. Why Do the ICU Team Wants Her To Be Discharged?