


Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS
Hi, it’s Patrik Hutzel from INTENSIVECAREHOTLINE.COM where we instantly improve the lives for Families of critically ill Patients in Intensive Care, so that you can make informed decisions, have PEACE OF MIND, real power, real control and so that you can influence decision making fast, even if you’re not a doctor or a nurse in Intensive Care!
This is another episode of “YOUR QUESTIONS ANSWERED“ and in last week’s episode I answered another frequently asked question from our readers and the question in the last episode was
You can check out last week’s episode by clicking on the link here.
In this week’s episode of “YOUR QUESTIONS ANSWERED“, I want to start answering questions from one of my clients James, which are excerpts from 1:1 phone and email consulting and advocacy sessions with me and the topic this week as part of a 1:1 consulting and advocacy session with me and one of my clients James is
What they don’t tell you in Intensive Care when it comes to weaning from tracheostomy and ventilation!
James contacted me last year in August and him and his family were facing a massive challenge. His Dad in his early 70s had a haemorrhagic stroke and he therefore had a massive bleed in his brain.
When John first contacted me his Dad had already spent a few weeks in ICU and already had a tracheostomy because he needed long-term ventilation in ICU.
Furthermore, John’s Dad wasn’t “waking up” due to the increased seizure medication he was getting, as part of his condition was that he had frequent seizures to begin with.
To make matters worse, besides the stroke, the seizure activity and the long-term ventilation, the ICU was adamant to send his Dad out of ICU into LTAC (long-term acute care.) If you have followed my consulting and advocacy for any length of time you would know that I strictly advice against LTAC or subacute care.
I can’t tell you how many people contact us in desperation when they have a loved one in LTAC and want to get them back into ICU. LTAC’s are disaster at the best of times.
Cutting to the chase, in this series of 1:1 consulting and advocacy sessions with my client James, I can show him how to keep his Dad in ICU against the hospital’s wishes and I can show James how he can negotiate best care and treatment for his Dad, including getting him off the ventilator and the tracheostomy as well as managing the seizures!
Enjoy today’s consulting and advocacy session.
James: Hi Patrik.
Patrik: Hi James. How are you?
James: What time is it there?
Patrik: Close to midnight. That’s OK. I just, I just got your email.
James: So yeah, I wanted to talk and touch base with you on a few things.
So those were his ventilator setting last night. He was breathing on his own most of the day yesterday. I actually, I only have about 10 minutes or 12 minutes, because I have a conference call here pretty soon, but um, so those were the ventilator settings that I just sent you.
He was up in the chair for I think two and a half, maybe even three hours. And you know, he made some pretty good progress in the chair, you know, even just weeping for a while, but it takes a lot to really wake him up or once you wake them up and keep him going. He was very responsive and very active and you know, the more I explain things to him about what happened to him and you know, that he needed to follow my commands in order to get them out of the hospital and started following my commands more.
Related article/video:
James: It makes sense because if you’re, yeah, if you’re just sitting there and someone keeps saying, Hey, lift your arm, you’re here and you’re tired, you’re probably, he’s not going to do it. Um, but after I explained him the reasons why I keep asking and saying, Gee, he did it more often and he’s very tired. He was very fatigued, is multiple. We’re starting to atrophy more than anything. Um, those were the ventilator settings. And then we went to, we went to this LTAC (Long-term acute care facility) yesterday to look at it, right? The place is complete pile of shit. I don’t, I don’t feel comfortable at all.
Patrik: Right.
James: These people have been lying to us, you know, basically saying that the LTAC is really an extension of the Cleveland Clinic, guess what, it’s not! It’s a completely separate place.
They don’t have the same doctors. My father is still way too critical to, uh, to move him to an LTAC. I need to figure out a way to keep him here. And you know, they. This is the second biggest Rehab hospital in the United States of America. They should have the facility and the resources to keep him here to wean him off his ventilator and start his rehab and get him stabilized and they shouldn’t just kick them out of the ICU. And then go to an LTAC.
Patrik: You’re absolutely right!
James: It’s not why I brought him here. No, no bullshit. So yeah, I need to figure out a way to, for him to keep him here. Do you have any suggestions?
Patrik: Yeah. The first thing that stands out with this picture that you sent, right?
There’s a big, huge difference. Huge improvement to the last picture that you sent. So just by that he’s very close to having time off the ventilator, he is very close.
So to put that in perspective, if he had a breathing tube and not the tracheostomy right and on those settings, if he had a breathing tube and would obey commands and he could swallow, which is why he’s got the tracheostomy in the first place, those would be… He would be ready to come off the ventilator on those settings if you had a breathing tube and he could swallow. OK. So from that perspective…
James: Hold on, hold on…
- So you’re saying if he had a breathing tube, he’d be ready to come off of it?
Patrik: Yeah, that means he will have time off the ventilator soon in the next few days. I would, I would argue in the next 24 to 48 hours. If they’re not taking him off the ventilator in the next 24 to 48 hours if they’re not putting him on the tracheostomy collar, they’re dropping the ball. Right?
James: OK.
Patrik: So because and that leads me to the LTAC (long-term acute care facility)
That’s what I always…well what I said from the start, any ICU is much better equipped to get a patient off the ventilator than any LTAC ever is, right?
So that that’s why you sort of got to keep asking now. OK, when we’ll he have time off the ventilator right, because he’s close. Right?
So that’s what I would be pushing for if I was you. I can’t see why they… yeah, go on.
James: What is the tracheostomy collar again real quick?
Patrik: Basically all they do is they take your dad off the ventilator and they put him on humidified oxygen. Right. And the humidification. That’s all it is.
James: OK, it’s a collar?
Patrik: Yeah. It’s a collar and the actual humidification and oxygen, will go through the collar into the tracheostomy. That’s what it is. Nothing spectacular
James: Got you, humidity because he’s not breathing through his nose?
Patrik: That’s exactly right.
James: Based on the settings do you think he’s ready to come off the ventilator now? Do you think he’s ready now?
Patrik: Very, very much so. And especially if he’s sitting up, that’s the time when they need to do it because that’s easiest for him.
James: OK.
All right. Sounds good. Um, if they, if they insist, so if they take him off the ventilator and he can stay off it, he’s gonna go to step down. He’s not going to go the LTAC is he?
Patrik: Well, I mean the longer you can stay in this hospital, if you can avoid the LTAC and he can go to step down and then to neuro rehab that I belief is the preferred option. Especially, you know, I’m sure in Cleveland there would be more than one LTAC, but you know, you’ve seen one and the place didn’t instil any confidence in you. Right? So, you know, um, you know, that the hospital for now is the best place.
James: I can’t even believe that they even suggested LTAC, there was only one doctor in the whole building when we went there.
Patrik: I’m not surprised. Sorry. I’m not surprised. Not surprised at all.
James: I mean, you know, I’m going from, I’m going from one of the best hospitals in the world where there’s five doctors every night, you know, to a, to a building where there’s one doctor on five floors and then it’s like a, it’s like a nursing home and my Dad just had brain surgery four weeks ago.
Recommended:
Patrik: No, no, no, no. He’s not ready.
So, you know, I think, I think your next steps really are to say, you know, when, when do we be having time off the ventilator and when will he be on the tracheostomy collar, that those are your questions for them. Um, don’t be discouraged if your Dad can only stay off the ventilator for an hour or for two hours every day to begin with. That might happen. If it does happen, don’t be discouraged. It’s a start. If he can, you know, in the ideal world they can have him off the ventilator for two hours and then onwards, you know. And that would be, that would be a good start too. But again, don’t be discouraged if there are any setbacks, you know, it doesn’t necessarily happen straight away, but what needs to happen straight away, they need to try him off the ventilator. That definitely needs to happen today.
James: So to begin with, on and off for two hours or two hours a day as well?
Patrik: As I said they need to start, you know, at first to begin with to take him off for an hour and see what happens. That’s the first step. They will, should get a good idea within an hour. How he tolerates that? And if he tolerates it, well let’s keep it well for a couple of hours but then probably put it back on. You don’t want to overdo it in the beginning, but you know, you know, say, say they’d take him off from 10:00 AM to 11:00 AM. Give him a break, you know, over the lunch period. And then maybe take him off again from 3:00pm to 4:00 PM. If he can tolerate that on his first day where they’re trialling him off the ventilator, that would be a big step. And then tomorrow, you know, put him in the chair and then we also try to put him in the chair today, or is that already happening?
James: Oh No, no, no, no, not at all. I think that’s what they need to aim for because it’s much easier for him to breathe by himself while he’s sitting up.
Patrik: They’ll put him in the chair and take him off.
James: Yeah, OK. Can he die from being taken off the ventilator?
Recommended:
Patrik: No, he can’t and the reality… and that’s what I mean, it’s a trial and if he can’t…if he can’t tolerate it, they can see that very quickly and they put him back on the ventilator. That’s it. No big deal. What happens is he will start breathing very quickly. He might, he might, he might start breathing very fast and he might drop his oxygen levels, but they will see that very, very quickly.
James: OK. All right. That’s good advice. That’s good advice. So you think that with these ventilator settings that he’s very close to come off it with what you see there?
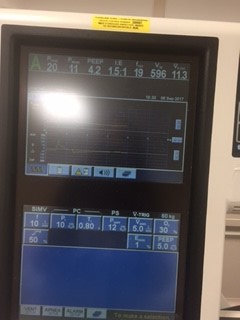
Patrik: Yep. So number one, he is breathing spontaneously. OK. So He’s breathing 23 breaths per minute on the screen. The screen you’ve shown me on when we spoke last, he had 10 breaths from the machine and he was breathing nine breaths by himself and therefore he was getting 19 breaths per minute in total and now he’s breathing 20 by himself. So that’s fairly similar to that. That’s number one. See The 6:25. Can you see that? The volume?
James: Yeah, that’s good.
Patrik: That’s a good volume. And do you remember on the last screen there was about 600 mls and that was with more support from the machine. So that’s with less support and he’s breathing about the same if not more. So that’s a good sign. The PEEP of five is a PEEP where you would extubate, like, you know, if he had a breathing tube, you could take the breathing tube out on a PEEP of five. Um, you can see 30 percent of oxygen. That doesn’t need to be any lower than that. OK. Um, you can see on the top, not on, can you see the 10 where it says PS so you see the 30 percent of oxygen and to, two quarters on the left, it’s just 10 pressure support. Can you see it?
James: Uh, yes. Right.
Patrik: So that’s the pressure support. You know, you can usually extubate on 10 on a pressure support.
James: Yeah.
Patrik: OK. So that’s pretty, that’s a good number. And I argue they can wean that down to eight even because his volume is also good. If his volumes before hundred on a pressure support of 10, I’d say he’s not ready, but with the volume of 625 with a pressure support of 10, that’s pretty good.
James: What do you mean by volume? Yeah, what does that mean?
Patrik: Yeah, the volume is basically. So you can see it on the top of the screen. The 625.
James: Yes. Right.
Recommended:
Patrik: So that’s basically 625 mls and that’s basically the volume he inhales. Does that make sense?
James: Like your volume of air?
Patrik: Yeah, volume of air. Does that make sense?
James: Yes.
Patrik: Literature and research suggests on average seven to 10 mls per kilo. I know you, you are not in the metric system. Right? But your dad is about. I think we’ve talked about this. Eighty three kilos. I know you’ve told me in stones, but I’ve done the calculations. It’s about 83 kilos. So for simplicity, 10 mls times 830 mls, but let’s say seven to 10 mls. So that’s, that’s a, that’s a really good number.
James: OK. All right, well that’s good advice for today. So I’m going to ask them to put him up in the chair and then ask them to, to get him on the tracheostomy collar!
Patrik: Absolutely!
James: And if we can get to a step-down unit. Do you have any idea how long my Dad might stay in a step down unit?
Patrik: No. It also depends what skill level they have on the step-down unit, right? Some step-down units might take your dad while he’s still on the ventilator, other step-down units can’t look after ventilators. So it really depends on the skill level they have on this step-down unit.
James: I’m sure that they know how to do it.
Patrik: Right.
James: He seemed to be, he seemed to be making pretty good progress.
Patrik: It really sounds like it. It really sounds like it.
James: How long do you think it will take to get him off the ventilator?
Patrik: Yep. So there is no one size fits all. OK? Some patients come off really within 24 to 48 hours. Others might take a couple of weeks and others might take even a few months. Right? That’s why I’m saying don’t be discouraged if you know, if he might fail on his first attempt!
Recommended:
James: Even if he’s breathing on his own right now?
Patrik: Oh yeah. Yeah. It could. That, that’s the worst scenario. That’s the worst case scenario I’d tell you. I tell you sort of a, a typical sort of pathway if you will, you know, as I say, they tried him very slowly, you know, a couple of hours for the next couple of days. If he can tolerate that, hopefully they can expand that to take him off the ventilator during the daytime and then maybe ventilating overnight for the next few days and once they know he can stay off the ventilator during the day then it’s time to trial and keep him off overnight as well!
James: Ok great, that’s good advice, I need to go, I need to get on a conference call with my wife, I’ll call you back in half an hour!
Watch out for the next consulting session with James in the next episode of “YOUR QUESTIONS ANSWERED”/
See you then!
Your friend,
Patrik
You can also read or watch other parts of this 1:1 consulting and advocacy with James and his sister Christine here
How can you become the best advocate for your critically ill loved one, make informed decisions, get peace of mind, control, power and influence quickly, whilst your loved one is critically ill in Intensive Care?
You get to that all important feeling of making informed decisions, get PEACE OF MIND, CONTROL, POWER AND INFLUENCE when you download your FREE “INSTANT IMPACT” report NOW by entering your email below!
In Your FREE “INSTANT IMPACT” report you’ll learn quickly how to make informed decisions, get PEACE OF MIND, real power and real control and how you can influence decision making fast, whilst your loved one is critically ill in Intensive Care! Your FREE “INSTANT IMPACT” Report gives you in-depth insight that you must know whilst your loved one is critically ill or is even dying in Intensive Care!
Sign up and download your FREE “INSTANT IMPACT” REPORT now by entering your email below! In your FREE “INSTANT IMPACT” REPORT you’ll learn how to speak the “secret” Intensive Care language so that the doctors and the nurses know straight away that you are an insider and that you know and understand what’s really happening in Intensive Care! In your FREE report you’ll also discover
- How to ask the doctors and the nurses the right questions
- Discover the many competing interests in Intensive Care and how your critically ill loved one’s treatment may depend on those competing interests
- How to eliminate fear, frustration, stress, struggle and vulnerability even if your loved one is dying
- 5 mind blowing tips& strategies helping you to get on the right path to making informed decisions, get PEACE OF MIND, control, power and influence in your situation
- You’ll get real world examples that you can easily adapt to your and your critically ill loved one’s situation
- How to stop being intimidated by the Intensive Care team and how you will be seen as equals
- You’ll get crucial ‘behind the scenes’ insight so that you know and understand what is really happening in Intensive Care
- How you need to manage doctors and nurses in Intensive Care (it’s not what you think)
Thank you for tuning into this week’s YOUR QUESTIONS ANSWERED episode and I’ll see you again in another update next week!
Make sure you also check out our “blog” section for more tips and strategies or send me an email to [email protected] with your questions!
Also, have a look at our membership site INTENSIVECARESUPPORT.ORG for families of critically ill Patients in Intensive Care here.
Or you can call us! Find phone numbers on our contact tab.
Also check out our Ebook section where you get more Ebooks, Videos and Audio recordings and where you can also get 1:1 counselling/consulting with me via Skype, over the phone or via email by clicking on the products tab!
This is Patrik Hutzel from INTENSIVECAREHOTLINE.COM and I’ll see you again next week with another update!
Related Articles:
- 5 Ways to have control, power and influence while your loved one is critically ill in Intensive Care
Related Articles:
 MY HUSBAND OF 24 YEARS WAS IN ICU AFTER CARDIAC ARREST AND HE DIED! IT WAS HORRIBLE AND I THINK HE COULD HAVE BEEN SAVED WITH A MORE POSITIVE INTENSIVE CARE TEAM!
MY PARTNER IS IN INTENSIVE CARE ON A VENTILATOR! THE INTENSIVE CARE TEAM WANTS TO DO A TRACHEOSTOMY AND I WANT TO HAVE HIM EXTUBATED! WHAT DO I DO? (PART6)
My boyfriend has Pancreatitis and is in Multi-organ failure, how long will it take for him to get out of Intensive Care? (PART2)
My brother is in ICU with cardiac arrest, abdominal sepsis, ventilated and in an induced coma, will he need a tracheostomy?
My uncle is in Multi-organ failure after three weeks in ICU! He’s ventilated with a trachea, on Haemodialysis and he’s not waking up! Everything seems to go wrong, what do we need to do?
MY HUSBAND OF 24 YEARS WAS IN ICU AFTER CARDIAC ARREST AND HE DIED! IT WAS HORRIBLE AND I THINK HE COULD HAVE BEEN SAVED WITH A MORE POSITIVE INTENSIVE CARE TEAM!
MY PARTNER IS IN INTENSIVE CARE ON A VENTILATOR! THE INTENSIVE CARE TEAM WANTS TO DO A TRACHEOSTOMY AND I WANT TO HAVE HIM EXTUBATED! WHAT DO I DO? (PART6)
My boyfriend has Pancreatitis and is in Multi-organ failure, how long will it take for him to get out of Intensive Care? (PART2)
My brother is in ICU with cardiac arrest, abdominal sepsis, ventilated and in an induced coma, will he need a tracheostomy?
My uncle is in Multi-organ failure after three weeks in ICU! He’s ventilated with a trachea, on Haemodialysis and he’s not waking up! Everything seems to go wrong, what do we need to do?