


Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS
Hi, it’s Patrik Hutzel from INTENSIVECAREHOTLINE.COM where we instantly improve the lives for Families of critically ill Patients in Intensive Care, so that you can make informed decisions, have PEACE OF MIND, real power, real control and so that you can influence decision making fast, even if you’re not a doctor or a nurse in Intensive Care!
This is another episode of “YOUR QUESTIONS ANSWERED“ and in last week’s episode I answered another question from one of my clients and the question in the last episode was
You can check out last week’s episode by clicking on the link here.
In this week’s episode of “YOUR QUESTIONS ANSWERED“, I want to continue answering the next question from one of my clients Emma, which are excerpts from 1:1 phone and email counselling and consulting sessions with me and the question this week is
My sister is in ICU on a balloon pump and ventilated after cardiac surgery! The ICU doctors want to stop treatment against our wishes and let her die, what should we do? (PART 15)
You can also access previous episodes in this series of questions here PART1, PART2, PART 3, PART 4, PART 5, PART 6, PART 7, PART 8, PART 9, PART 10, PART 11, PART 12, PART 13 and PART 14 by clicking on the relevant links.
In this series of 1:1 phone and email consulting and advocacy sessions with my client Emma you’ll get real in-depth knowledge about cardiac failure in Intensive Care, how it works, the treatment and therapy options, how to wean somebody off the ventilator and most importantly, you’ll discover how to not take “no” for an answer and get strong advocacy.
You’ll witness how I can lead Emma in going from the Intensive Care team trying to coerce her and her family to agree to a “withdrawal of treatment” as being “in the best interest” for her sister to challenge that and the Intensive Care team having to do everything within their power to safe her sister’s life and turning the dynamics upside down in Emma’s favour.
That’s what happens when you have the right advice from a professional who knows Intensive Care inside out and who knows how to manage the dynamics and who can take the fear away of being intimidated by the Intensive Care team!
Enjoy this consulting and advocacy session!
Patrik: Okay. Do you think she’s comfortable on the tube?
Emma: No, I know she don’t want that tube.
Patrik: Okay. Okay. No, no, of course not. Okay. Have they stopped the fentanyl as well, do you know?
Emma: Have they…oh yes, they stopped that, but they give it through a syringe and push it in her IV. It’s not in the machine anymore where-
Patrik: Okay.
Emma: It automatically goes in.
Emma: Okay. When it comes to strengthening her heart, how could they do that?
Patrik: Yeah.
Emma: How could that happen?
Patrik: Rest, rest, rest. The heart, there’s not much they can do to speed up the recovery of the heart besides resting and supporting. She also needs the aortic valve replacement, but she’s too weak for having surgery, which is why they are reluctant to operate on her. The risk she could die on the operating table is too high at present especially with the inotropes and the vasopressors still going.
Emma: Okay.
Patrik: There is, the ECMO, would’ve still been an option, but for now, if they can maintain the vasopressin and the norepinephrine, that’s fine for now. That’s fine for now. I do strongly believe that if they can’t extubate her and if they can’t wean your sister off the inotropes/vasopressors she will need to be considered for ECMO and for potential heart transplant, but we’ll reassess tomorrow.
Emma: Okay.
Patrik: You know she needs to rest and it’s like she would’ve had a major event in the heart. Have they mentioned she had a heart attack? They haven’t mentioned that, have they?
Emma: They haven’t mentioned that.
Patrik: Right, right. That’s okay. Have they mentioned that she’s got cardiomyopathy? Have you heard of that?
Emma: No, I’ve heard of it, but they haven’t mentioned that.
Patrik: Okay.
Emma: No they didn’t. They said that aortic stenosis…
Patrik: Okay, yes, which is why she needs the aortic valve replacement.
Emma: So, nothing like a cardiomyopathy.
Patrik: Okay.
Emma: What is that?
Patrik: It’s a muscle weakness of the heart. But, if they haven’t mentioned that…I know that aortic stenosis has been the reason, but I’m just trying to find out have they investigated further? Have they been transparent with you? Have they mentioned something that you weren’t quite sure what it means? All of that.
Emma: Oh, okay. No, they haven’t mentioned that.
Patrik: Okay. No, no, that’s okay. Look, a recovery or a situation like that, is often two steps forward and one step back. I like that they are ambitious in taking her off the ventilator. I like that. It needs to happen. The time frames around that, I’m not 100% sure, right? She doesn’t need-
Emma: Okay.
Patrik: She doesn’t need to be off the vasopressin and the norepinephrine to be off the ventilator. That’s not necessarily a requirement. She needs to be awake even though it would be better if she was off the norepinephrine and the vasopressin to come off the ventilator and more importantly stay off the ventilator.
Emma: Okay.
Patrik: And she needs to breathe spontaneously on the ventilator. Both are the requirements. Now the dexmedetomidine makes it much more likely that she can, that she’s waking up more and more. That’s good. Whether she will be strong-
Emma: Okay.
Patrik: Whether she will be strong enough tomorrow, let’s wait and see. We don’t know yet. Okay?
Emma: Okay.
Patrik: All you can do at the moment is take one day at a time. What’s good to know as well is, you know her brain is intact.
Emma: Okay.
Patrik: That’s important to know.
Emma: Yeah.
Patrik: A lot of patients wake up and their brain is funny, right? They’re not responding appropriately, so that’s not the case. You’re sister, you think, is appropriate.
Emma: Okay.
Patrik: That’s good. Okay? That’s all increasing her chances of her doing all the right things, because she’s appropriate. That’s all good. And all you can do now is wait for another day. They are doing all the right things now.
Emma: Okay, okay. Thank you so much.
Patrik: You’re very welcome. You’re very welcome. Do you know whether she had an ultrasound of the heart in the last 48 hours? She must’ve had.
Emma: No, but I’ll…tomorrow.
Patrik: Okay. Tomorrow? Good. Because when they do that tomorrow, they will get an ejection fraction again.
Emma: Okay.
Patrik: Okay? So they will get another ejection fraction and they will just a better idea, you know, has her heart recovered more. You can get some of that, whether or not the heart is recovering, from how much vasopressin and how much norepinephrine she’s using, but, the ultrasound will be a very good tool, as well.
Do you know-
Emma: Okay.
Patrik: Do you know whether she’s, what they’re doing with the dobutamine? Do you know whether they’ve changed that?
Emma: No, the dobutamine has stayed the same. It’s still at five.
Patrik: Five. Okay. Okay. Alright. Okay. I’ll tell you what-
Emma: What I do know is that-
Patrik: Look, I’m not surprised that they haven’t reduced it. I’m not surprised. Okay? That’s a sign the heart is still weak. Okay? The minute, the vasopressin and the norepinephrine, I’m not too worried about at the moment. That’ll probably go up and down for the next few days. The one thing that I would like see going down in the dobutamine. That’s the one thing that I would like to see going down, but it’s not there yet.
Emma: Okay.
Patrik: But, again, it’s not the end of the world. It just means she’s not ready yet. We’ve gotta wait.
Emma: Okay. Okay.
Patrik: I’m very positive now that they are now doing all the right things. They’ve changed the propofol to the dexmedetomidine, they tried her breathing spontaneously, she hasn’t done that yet, that’s okay. They tried. With the dexmedetomidine, she will be getting more awake hopefully, so that’s increasing her chances of starting to breathe by herself and then we’ll see what happens.
Emma: Okay.
Patrik: Then we’ll see what happens next. But, I’m positive they’re doing all the right things. Now that we know they’re doing all the right things, and now that we know they’re a bit more friendly with you, keep re-engaging them, too.
Emma: Okay. I will do that.
Patrik: The minute you think it’s not going in the right direction, the minute you think they’re not transparent, the minute you think they’re not acting in your sister’s best interest, that’s when we will reassess.
Emma: Okay. Okay.
Patrik: Does that make sense?
Emma: It makes good sense. And then with that VSP on that breathing machine, what’s the difference in that with and that with the screen with the little lungs on it?
Patrik: At the moment, she is not breathing by herself. She’s getting some breathes from the machine. Now, I’m just bringing this up so I have it in front of me. Just give me one more sec. So, what did you mean with the little, what?
Emma: At first, on the breathing machine-
Patrik: Yeah.
Emma: There was a picture of lungs, but then the screen now don’t have the little lungs on it.
Patrik: Okay.
Emma: She said something about PSV?
Patrik: Yeah, PSV, PSV. PSV basically means she’s breathing by herself. Okay? Whereas the SIMV, the pictures you sent me, you only sent me SIMV. I didn’t get a picture from PSV. But that’s okay, I know- PSV stands for Pressure support ventilation and in essence that means she’s breathing by herself with a little pressure from the ventilator, but she needs to trigger every breath herself! SIMV on the other hand means she’s getting a set rate of breaths per minute and she can breathe on top of that. In the picture you sent me, she was getting 10 breaths/minute from the machine and she was breathing another 17 on top of that. She probably needs to be more awake and also a little stronger to get into PSV, which will get her close to being extubated.
Related article/video:
Emma: Oh, no, no, it’s SIMV, it’s not, it’s the one I sent, it’s the SIMV.
Patrik: Yeah. SIMV. I can’t see a little lung on the picture. Hang on, just give me one more sec. Just give me a sec. I can’t see a lung, a little lung on the picture.
Emma: Oh no, the lung is not on that picture, the lungs are not on that one.
Patrik: No.
Emma: They changed the screen.
Patrik: Yeah, they’ve changed the screen. So what it means at the moment, Emma, is she’s not breathing by herself 100%, right? But that’s okay. From what you’re telling me, they have tried the…no, no, hang on, no, no, she is breathing by herself. She is breathing by herself. No, no. She’s breathing by herself, however, so, have you got the picture in front of you?
Emma: Okay, let me pull it up.
Patrik: Thanks. Let me explain that, I’ll explain it to you.
Emma: Okay, I have it pulled up now.
Recommended:
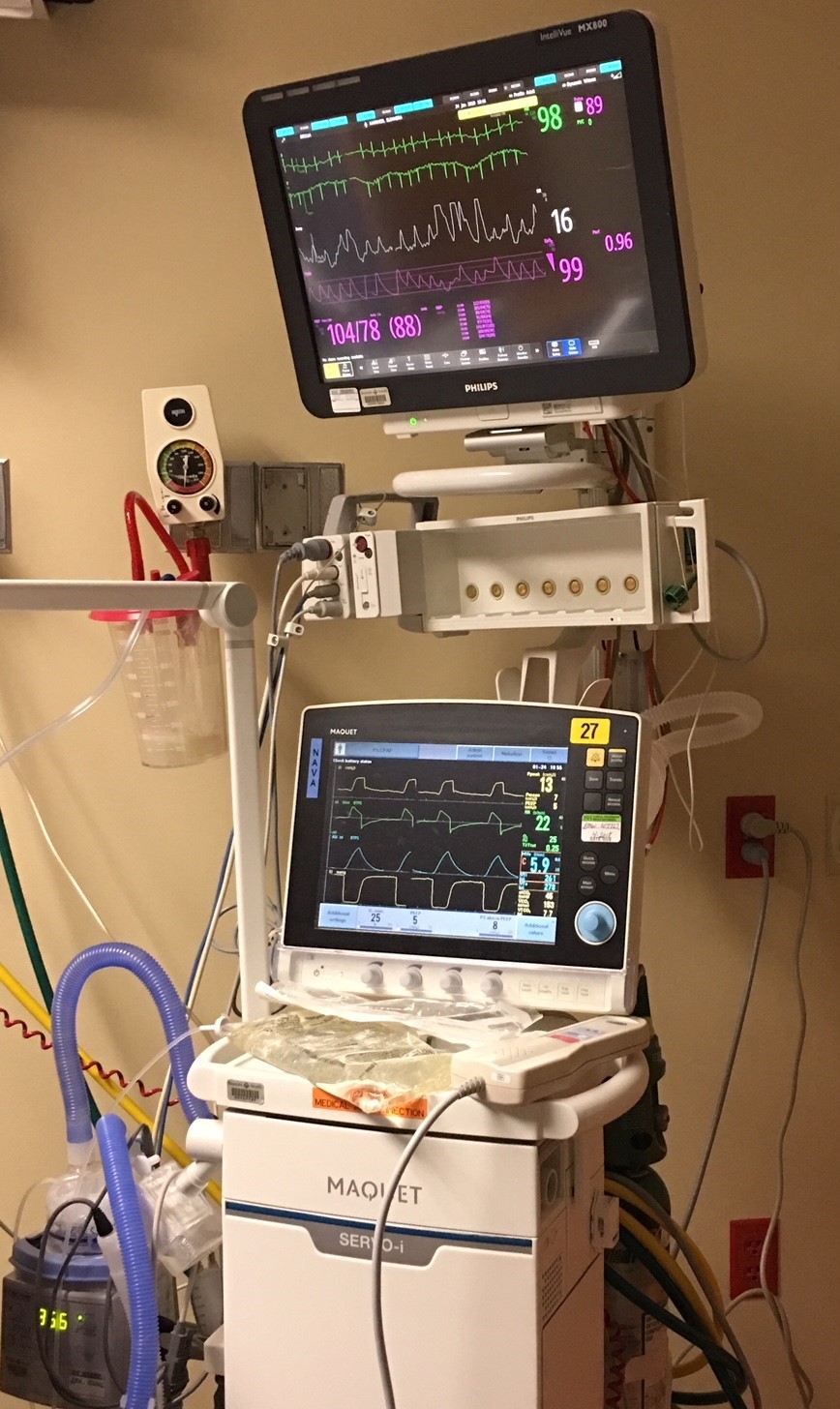
Patrik: Okay. So, hang on just give me one sec. Yeah. So, if you, on the left hand side, you can see, on the top left hand side, you can see the 7.9?
Emma: Uh huh.
Patrik: And then below that, you can see 286. Can you see that?
Emma: Uh huh. Yes.
Patrik: So, the 286 is the volume of her breath. So, she’s basically taking 286 mls per breath. Okay? How big is your sister, if I may ask? What’s her weight, roughly?
Emma: She’s probably about 240, if that.
Patrik: 240, what is-
Emma: 240. Pounds. Maybe 240? I’m not sure of her weight.
Patrik: Okay, that’s okay. Just give me one sec. Okay. Let’s just say 240 pounds, that’s fine. You can see with the 286 in the screen, that’s not enough. It would have to be somewhere around 600 to 1000 mls. Okay?
Emma: Okay.
Patrik: That’s not enough. While she’s breathing with minimal support from the ventilator, those volumes need to be bigger.
Emma: Okay.
Patrik: Okay? That’s a sign, yes, she can breathe by herself, but she’s not breathing large volumes as of yet. So she can’t take a deep breath yet.
Emma: Okay.
Patrik: Okay? But, if you look on the screen again, can you see the 17 spont when you go down that line? And then you can see the 10 BPM?
Emma: Yes, I see it.
Patrik: Yeah. So she’s, at the moment, she’s taking 27 breaths per minute in total. Okay? It means she’s getting 10 breaths per minute guaranteed from the machine and she’s now also taking 17 breaths by herself spontaneously, making it 27 breaths per minute in total.
Emma: Okay.
Patrik: And she’s taking-
Emma: And that’s on her own?
Patrik: 17/minute On her own. 10 breaths/minute from the machine and 17 by herself with a little bit of PS (pressure support).
Emma: Okay.
Patrik: Once she triggers a breath, yes, she will get some support from the ventilator, but it’s minimal.
Emma: Okay.
Patrik: Okay? It’s minimal. With that, ideally, instead of the 286 on the top, that number would be, let’s just say 600 or 700, okay? And, that would bring the 27 down to maybe 15 or 20, because she-
Emma: Oh, okay. Okay, I understand.
Patrik: Because she would breathe a lot slower with bigger volumes.
Emma: Okay.
Patrik: Right? At the moment, she’s probably trying to overcompensate. She’s probably trying to overcompensate because she most likely has a relatively high CO2 (Carbondioxide). They could see that in her arterial blood gas (ABG). If her CO2 was normal they could most likely get her to breathe in PSV and she would be much closer to extubation.
Emma: Okay.
Related article/video:
Patrik: But that’s okay. The good news is, she’s breathing by herself at least for some part. That’s the good news.
Emma: Okay.
Patrik: Right?
Emma: Right.
Patrik: Again, she’s not there yet, but she’s more awake, she’s breathing by herself, and yes, the vasopressin and the norepinephrine is still up and down, but that’s okay for now. She’s making, again, baby steps. Baby steps, but steps.
Emma: Okay.
Patrik: I’d say we’ll reassess tomorrow.
Emma: Okay.
Patrik: Yeah. Any questions you have in the meantime, give me a call or flick me an email.
Emma: Okay. I got you. I will.
Patrik: Is there anything else you want to know?
Emma: No, that’s it. That’s it for now. I’m just taking it…when I walked in there and heard all that news, it kind of was a downer. My sister’s, saying she’s fighting, I’m not in denial, I’m just hoping and praying that, believing that she’s going to recover, so one day at a time. One day at a time.
Patrik: Yeah. Absolutely. Just remind me again, how old is your sister again? 56?
Emma: Yes.
Patrik: Yeah, that’s very young. The younger people are, the higher the chances of recovery. There’s never a guarantee, but one way or another, she deserved another chance. That’s the most important thing.
Emma: Yes.
Patrik: They would’ve just stopped everything on the weekend.
Emma: Yeah.
Patrik: The other good sign is she was on the balloon/IABP. Now, when you remove the balloon, you can usually only do that if the heart is strong enough to cope.
Emma: Oh, okay.
Patrik: So, yes, she has the vasopressors/inotropes still going, but very few patients come off the balloon/IABP without the vasopressors. She’s not, she’s coped, with getting off the balloon/IABP, yet she needs the vasopressors and the dobutamine, but that’s normal.
Emma: Okay, okay.
Patrik: You remember, they were telling you that she can’t come off the balloon? Well that’s not accurate. She is off the balloon/IABP, and she’s alive.
Emma: Yes, yes.
Patrik: She’s come a long way, against their predictions.
Emma: Yes.
Patrik: To put it all in prospective, it’s a puzzle. It’s a puzzle.
Emma: It is. It is. Yes.
Patrik: You’ve gotta keep looking after yourself. That’s very important.
Emma: Yeah, but it’s hard because-
Patrik: I know.
Emma: I feel like I’m just stuck. I can’t move until…I’m just stuck until she come out of this.
Patrik: It’s very difficult, and you’re doing very well, but you need to pace yourself. You need to pace yourself.
Emma: Okay, I will do that.
Patrik: Also, if you feel like you wanna have a day off, not go to the hospital, I’m very happy to talk to some of your other family members. I’m very happy to do that, if you feel like-
Emma: Okay, okay.
Patrik: Very happy to do that. There’s no restrictions.
Emma: Okay, okay. Thank you, so much.
Patrik: You’re very welcome. You’re very welcome.
What I’ll do. I can’t do it right now, but for you, its night time, when you get up in the morning, I will send you another email, just with quickly summarising what we discussed. Then you have it in front of you-
Emma: Okay.
Patrik: And then you have it front of you again.
Emma: Okay, okay.
Patrik: Let me know what’s next, what you need next then.
Emma: Okay, okay. Thank you so much.
Patrik: You’re very welcome. You’re very welcome. Take care for now.
Emma: Okay.
Patrik: All the best.
Emma: Okay, okay. Thanks.
Patrik: Bye.
Emma: Bye-bye.
Patrik: Bye-bye.
How can you become the best advocate for your critically ill loved one, make informed decisions, get peace of mind, control, power and influence quickly, whilst your loved one is critically ill in Intensive Care?
You get to that all important feeling of making informed decisions, get PEACE OF MIND, CONTROL, POWER AND INFLUENCE when you download your FREE “INSTANT IMPACT” report NOW by entering your email below!
In Your FREE “INSTANT IMPACT” report you’ll learn quickly how to make informed decisions, get PEACE OF MIND, real power and real control and how you can influence decision making fast, whilst your loved one is critically ill in Intensive Care! Your FREE “INSTANT IMPACT” Report gives you in-depth insight that you must know whilst your loved one is critically ill or is even dying in Intensive Care!
Sign up and download your FREE “INSTANT IMPACT” REPORT now by entering your email below! In your FREE “INSTANT IMPACT” REPORT you’ll learn how to speak the “secret” Intensive Care language so that the doctors and the nurses know straight away that you are an insider and that you know and understand what’s really happening in Intensive Care! In your FREE report you’ll also discover
- How to ask the doctors and the nurses the right questions
- Discover the many competing interests in Intensive Care and how your critically ill loved one’s treatment may depend on those competing interests
- How to eliminate fear, frustration, stress, struggle and vulnerability even if your loved one is dying
- 5 mind blowing tips& strategies helping you to get on the right path to making informed decisions, get PEACE OF MIND, control, power and influence in your situation
- You’ll get real world examples that you can easily adapt to your and your critically ill loved one’s situation
- How to stop being intimidated by the Intensive Care team and how you will be seen as equals
- You’ll get crucial ‘behind the scenes’ insight so that you know and understand what is really happening in Intensive Care
- How you need to manage doctors and nurses in Intensive Care (it’s not what you think)
Thank you for tuning into this week’s YOUR QUESTIONS ANSWERED episode and I’ll see you again in another update next week!
Make sure you also check out our “blog” section for more tips and strategies or send me an email to [email protected] with your questions!
Also, have a look at our membership site INTENSIVECARESUPPORT.ORG for families of critically ill Patients in Intensive Care here.
Or you can call us! Find phone numbers on our contact tab.
Also check out our Ebook section where you get more Ebooks, Videos and Audio recordings and where you can also get 1:1 counselling/consulting with me via Skype, over the phone or via email by clicking on the products tab!
This is Patrik Hutzel from INTENSIVECAREHOTLINE.COM and I’ll see you again next week with another update!
Related Articles:
- 5 Ways to have control, power and influence while your loved one is critically ill in Intensive Care
Related Articles:
 My uncle is on BIPAP after two weeks on the ventilator and the doctors think that putting the breathing tube back in is futile! What does it mean?
My 47 year old sister is in ICU with Pneumonia and the Intensive Care team wants to “pull the plug”! Help! – INTENSIVE CARE HOTLINE
How long can a critically ill Patient stay on life support?
My uncle is on BIPAP after two weeks on the ventilator and the doctors think that putting the breathing tube back in is futile! What does it mean?
My 47 year old sister is in ICU with Pneumonia and the Intensive Care team wants to “pull the plug”! Help! – INTENSIVE CARE HOTLINE
How long can a critically ill Patient stay on life support?
 My 57 year old Dad has been in Intensive Care with Cardiomyopathy and Pneumonia for 5 weeks! He’s still in an induced coma and still doesn’t have a tracheostomy, HELP! (PART 7)
My 57 year old Dad has been in Intensive Care with Cardiomyopathy and Pneumonia for 5 weeks! He’s still in an induced coma and still doesn’t have a tracheostomy, HELP! (PART 7)
 My 57 year old Dad has been in Intensive Care with Cardiomyopathy and Pneumonia for 5 weeks! He’s still in an induced coma and still doesn’t have a tracheostomy, HELP! (PART 11)
My 57 year old Dad has been in Intensive Care with Cardiomyopathy and Pneumonia for 5 weeks! He’s still in an induced coma and still doesn’t have a tracheostomy, HELP! (PART 11)