


Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS
Hi, it’s Patrik Hutzel from INTENSIVECAREHOTLINE.COM where we instantly improve the lives for Families of critically ill Patients in Intensive Care, so that you can make informed decisions, have PEACE OF MIND, real power, real control and so that you can influence decision making fast, even if you’re not a doctor or a nurse in Intensive Care!
This is another episode of “YOUR QUESTIONS ANSWERED“ and in last week’s episode I answered another question from our readers and the question was
You can check out last week’s question by clicking on the link here.
In this week’s episode of “YOUR QUESTIONS ANSWERED“, as part of my 1:1 consulting and advocacy service, I want to answer the succeeding questions from one of my clients Caroline asking why her fiancé named Charly confined in the ICU, still needs a tracheostomy despite having his own breathing efforts, as told by the ICU nurses.
My Fiancé Is Breathing On His Own. Why do the ICU Nurses Keep On Saying He Still Needs a Tracheostomy?
Caroline: Yes, okay.
Tom: Okay.
Caroline: Alright, I guess, yes, it seems …
Patrik: You know what, if you can send me a picture of the ventilator, that would be very, very helpful, because then I can tell you how far away he is from being extubated,
Caroline: Oh, okay. Alright, well, all I know-
Patrik: That would be very helpful.
Caroline: He is consistently at 20. That’s all I … And he’s done more than that. The most he’s done is 34.
Patrik: Okay, do you know-
Recommended:
Caroline: But he’s been constant at 20.
Patrik: Okay, with the 20, do you know if that’s breath per minute?
Caroline: Yes, yes, and they have it more at 30.
Patrik: Right, do you know if that 20 breaths per minute, do you know whether that is breathing himself, or is that given by the machine? Do you know?
Caroline: That’s him by himself, that’s him by himself. I asked the respiratory therapist yesterday.
Patrik: Okay, well, well, that’s good. If it’s accurate, that’s good, because then he should be as close as coming off the ventilator as possible.
Recommended Links:
Caroline: Yes.
Patrik: Right.
Caroline: Yes, that’s what I thought, but the nurse told me today that, well, if his brain can’t tell his body to breathe, then that’s why we think he needs the tracheostomy, it’s what they told me.
Patrik: Sure. Do you know if he has an arterial line?
Caroline: What does that look like?
Patrik: Do you know whether they’re checking arterial blood gases or ABGs? Do you know whether they’re checking blood gases for oxygen levels or for carbon dioxide levels?
Recommended Links:
Caroline: That’s on the vent, right?
Patrik: No.
Caroline: That’s on the ventilator, right?
Patrik: No, it’s a blood test. It’s a blood test.
Caroline: Oh, I think they did mention that, but I can always just check.
Patrik: Yes, okay. That’s okay. Again, don’t worry too much about it for now. The most important thing is he’s breathing by himself, by the sounds of things.
Caroline: Yes.
Patrik: That means he should be as close to coming off the ventilator as possible. So then, the question is why can’t they extubate him, right? That would be my question.
Caroline: Yes, because they haven’t done him the trial. Okay.
Find information about weaning off the ventilator:
Patrik: That would be my question.
Caroline: Alright. So can I send you the picture in your email?
Patrik: That would be really great, that would be really great, because-
Caroline: Okay, I’ll do that now.
Patrik: Right, right. That would be really helpful.
Tom: Alright.
Patrik: And that is the question that Charly’s dad needs to ask them, “Why do you want a tracheostomy if he’s breathing by himself and he might be close to extubation?” That to me is the make or break question.
Caroline: Yes, okay.
Patrik: Right, and I-
Caroline: I will send the pictures.
Patrik: Yes, and I can tell you that from an ICU perspective, what it could be is yes, the risk that they take out the breathing tube and they may have to put it back in. Yes, that risk is a reality. There’s no doubt about that. But what they think is, “Okay, well, let’s do a tracheostomy, because that will make it safe for us to send Charly to long-term acute care.” Right? As I mentioned to you last week, the worst-case scenario from an intensive care perspective is to look after a patient indefinitely with an uncertain outcome, and Charly is in a situation like that.
Suggested Links:
Caroline: Yes, I understand. Okay.
Patrik: And also, just quickly, looking at timelines, the ICU is often trying to work with artificial timelines, and again, without looking at the individual’s needs. I mean, it’s ridiculous to say, “Oh, we only have two weeks for Charly to stay in intensive care.” That’s ridiculous. I mean, Charly might need four weeks. Who knows? We don’t know.
Caroline: Yes, yes.
Patrik: You know, so don’t-
Tom: Okay, so let’s-
Patrik: Don’t let other people impose any timelines on you.
Caroline: Okay.
Recommended links:
Caroline: Alright, thank you very much Patrik. I will get again the pictures right now for you and email you that.
Patrik: Yes, and then we can get back on the phone, okay?
Tom: Okay.
Patrik: Is this helpful so far?
Caroline: Yes, yes. It’s very helpful, yes.
Patrik: Okay, alright, look, send to me the picture and then I can call you back or I can click you back on email, and then we can use the remaining time when you want to.
Caroline: Okay, alright then. Thank you very much.
Patrik: You’re very welcome. It’s all the best for now.
Tom: Okay, thank you.
Patrik: Goodbye.
Tom: Goodbye.
Caroline: Goodbye.

Automated: For English, press one. Please enter your PIN … For more options, including …
Tom: Hello?
Patrik: Hi, Tom, it’s Patrik again, from Intensive Care Hotline.
Tom: Yes. How are you?
Patrik: I’m very good, thank you.
Tom: Mm-hmm (affirmative). I’m going to put Caroline on the phone.
Patrik: Yes.
Tom: Okay.
Caroline: Good. Hold on. Yes.
Patrik: Hi, Caroline. It’s Patrik here again.
Caroline: Yes, hi.
Patrik: Thank you for sending this through. To me, it looks like he’s not breathing by himself in there. Can you-
Caroline: Okay.
Patrik: Have you got the picture in front of you?
Caroline: No, I don’t-
Patrik: That’s okay.
Caroline: But, I can pull it up right now.
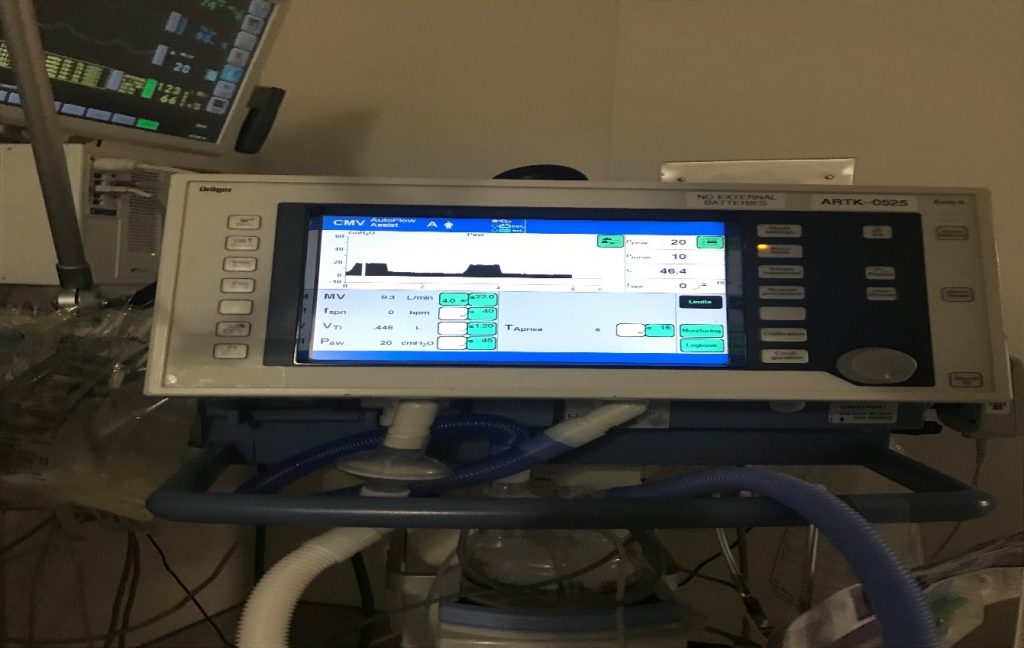
Patrik: That’s okay. That’s okay. There is, number one, the ventilation mode is CMV, which stands for controlled mandatory ventilation, which means it’s controlled and it’s mandatory, which means he’s getting mandatory breaths by the machine, okay?
Caroline: Okay.
Patrik: The other thing is, there is a section in the picture where it says S, spontaneous. It says FSPN. F stands for frequency, and SPN stands for spontaneous, and that section says zero.
Related links:
Caroline: Oh, I think I see that.
Patrik: So, with that information, I would think that he’s not breathing by himself, that this is … Everything is being done by the machine at the moment. Now, is this picture is from today?
Caroline: Yeah, yeah, it’s just now.
Patrik: Do you know whether he has been in those settings in particular for quite some time? Or have they changed the settings?
Caroline: I know they were changed, but I don’t recall right … Yeah, no, I don’t know what it was.
Patrik: And you wouldn’t know how long he’s been on those settings?
Caroline: These new ones, around … I don’t know, because they do it whenever they …
Patrik: Right. Right. So …
Caroline: I’m in the room.
Patrik: Right, okay. Okay, so from that perspective, for now, if he’s been on those settings for days and they haven’t changed, then there is a good chance that he may need a tracheostomy. But I would, in order to be certain, it’s probably good to ask the question; “Is he taking any breaths by himself?” Because, in that picture, he’s not. Right?
Caroline: Okay.
Patrik: And keeping in mind, this is a snapshot, but there could also be … It looks to me like he’s getting 20 breaths per minute from the machine every minute. Okay?
Caroline: Yeah.
Patrik: And you might have taken the picture a minute later, and he might take five breaths by himself, but that would still mean he’s getting 20 breaths from the machine. You mentioned-
Caroline: So that’s not enough?
Patrik: You see, you mentioned earlier you’ve seen it up to 35, up to 34, is that correct?
Caroline: Yeah.
Patrik: Right.
Caroline: But that was the highest I’ve ever seen it, but it was very short. The most I’ve seen it in a constant was about 24.
Patrik: 24, and that-
Caroline: But when I was on … That’s why it’s confusing to me because I spoke with the respiratory therapist yesterday, he said 20 was good. So that’s why it’s a little confusing now.
Patrik: So, you know, that’s what it looks like to me on the picture, that it’s all done by the machine, but it seems something you definitely need to ask again in case they change it. Because, if he is breathing by himself then the question is, “Well, why can’t they take it out?”
Suggested Links:
If he’s not breathing by himself, well then a tracheostomy might be the right thing to do, but then the question also is, “Why is he not breathing by himself?” Have they got an answer for that?
Caroline: Okay. Okay. So, should I ask the respiratory therapist when he comes in again those questions?
Patrik: I think so. I think so.
Caroline: Or should I just ask doctors that?
Patrik: No, no, no. I think you should.
Caroline: Okay.
Patrik: I think you should. You can also ask-
Caroline: Ask them.
Patrik: … You know, you should also be able to ask the nurse or the doctor. It’s probably … They all should know the answer. Yes, the respiratory therapist is making some of the decisions and is doing some of the work, but the doctors and the nurses should also know the answer to that question.
Recommended link:
Caroline: Okay. Well, I’ll wait for him. When he comes in, he does one tap, tap, and then leaves, so I’ll try to speak with him again.
Patrik: Right. Right.
Caroline: Yeah. Yeah. Charly is moving now, so …
Patrik: Okay.
Caroline: Okay.
Patrik: All right.
Caroline: All right, then.
Patrik: So, you can let me know then when you want to get on the phone again. As I said, I can be very flexible.
Caroline: Yeah, okay.
Patrik: Or if you want me, you know … If you are at the bedside, what you can do as well, if you are at the bedside, for example, and you have a doctor there, or a nurse there, or a respiratory therapist, I’d be very happy for you to pull out the phone if you can and call me, and I’m very happy to talk to them directly. That would be alright.
Recommended:
Caroline: All right, good. I can … okay, that number, the 410 number. Okay.
Patrik: Yup. Yes.
Caroline: Okay.
Caroline: All right, dad.
Tom: Okay.
Patrik: Okay.
Caroline: Okay, thank you.
Patrik: You’re very welcome.
Caroline: Mm-hmm (affirmative).
Patrik: Bye-bye.
Caroline: Okay.
Patrik: Bye.
Tom: Bye.
How can you become the best advocate for your critically ill loved one, make informed decisions, get peace of mind, control, power and influence quickly, whilst your loved one is critically ill in Intensive Care?
You get to that all important feeling of making informed decisions, get PEACE OF MIND, CONTROL, POWER AND INFLUENCE when you download your FREE “INSTANT IMPACT” report NOW by entering your email below!
In Your FREE “INSTANT IMPACT” report you’ll learn quickly how to make informed decisions, get PEACE OF MIND, real power and real control and how you can influence decision making fast, whilst your loved one is critically ill in Intensive Care! Your FREE “INSTANT IMPACT” Report gives you in-depth insight that you must know whilst your loved one is critically ill or is even dying in Intensive Care!
Sign up and download your FREE “INSTANT IMPACT” REPORT now by entering your email below! In your FREE “INSTANT IMPACT” REPORT you’ll learn how to speak the “secret” Intensive Care language so that the doctors and the nurses know straight away that you are an insider and that you know and understand what’s really happening in Intensive Care! In your FREE report you’ll also discover
- How to ask the doctors and the nurses the right questions
- Discover the many competing interests in Intensive Care and how your critically ill loved one’s treatment may depend on those competing interests
- How to eliminate fear, frustration, stress, struggle and vulnerability even if your loved one is dying
- 5 mind blowing tips & strategies helping you to get on the right path to making informed decisions, get PEACE OF MIND, control, power and influence in your situation
- You’ll get real world examples that you can easily adapt to your and your critically ill loved one’s situation
- How to stop being intimidated by the Intensive Care team and how you will be seen as equals
- You’ll get crucial ‘behind the scenes’ insight so that you know and understand what is really happening in Intensive Care
- How you need to manage doctors and nurses in Intensive Care (it’s not what you think)
Thank you for tuning into this week’s YOUR QUESTIONS ANSWERED episode and I’ll see you again in another update next week!
Make sure you also check out our “blog” section for more tips and strategies or send me an email to [email protected] with your questions!
Also, have a look at our membership site INTENSIVECARESUPPORT.ORG for families of critically ill Patients in Intensive Care here.
Or you can call us! Find phone numbers on our contact tab.
Also check out our Ebook section where you get more Ebooks, Videos and Audio recordings and where you can also get 1:1 counselling/consulting with me via Skype, over the phone or via email by clicking on the products tab!
This is Patrik Hutzel from INTENSIVECAREHOTLINE.COM and I’ll see you again next week with another update!
Related Articles:
- 5 Ways to have control, power and influence while your loved one is critically ill in Intensive Care
Related Articles:
 HOW LONG DOES IT TAKE TO COME OFF A VENTILATOR/ RESPIRATOR IN INTENSIVE CARE?
HOW LONG DOES IT TAKE TO COME OFF A VENTILATOR/ RESPIRATOR IN INTENSIVE CARE?
 Can a tracheostomy be reversed?
Can a tracheostomy be reversed?
 What are the chances of survival after a tracheostomy?
What are the chances of survival after a tracheostomy?
 My Husband In The ICU Is Doing Better? Why does the ICU team push towards Withdrawal of Treatment?
My Husband In The ICU Is Doing Better? Why does the ICU team push towards Withdrawal of Treatment?