


Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS
Hi, it’s Patrik Hutzel from INTENSIVECAREHOTLINE.COM where we instantly improve the lives for Families of critically ill Patients in Intensive Care, so that you can make informed decisions, have PEACE OF MIND, real power, real control and so that you can influence decision making fast, even if you’re not a doctor or a nurse in Intensive Care!
This is another episode of “YOUR QUESTIONS ANSWERED“ and in last week’s episode I answered another question from one of my clients and the first question from Natasha in last week’s episode was
You can check out last week’s question by clicking on the link here.
In this week’s part 2 episode of “YOUR QUESTIONS ANSWERED“, I want to answer the questions from one my clients RICHARD as part of my 1:1 consulting and advocacy service!
Richard’s mother suffered from a fractured bone due to a fall. His mother was then transferred to the ICU due to cardiac arrest and had a tracheostomy during her stay at the ICU.
The ICU team is not following the policy regarding the treatment protocols for my mother. How can I respond to this?
“You can also check out previous 1:1 consulting and advocacy sessions with me and Richard here.”
Hi Richard,
Here is a quick summary of what we discussed over the phone
- Mindset
- Some games in life you don’t play in order to win
- It’s none of your business what other people think about you
- Don’t overcomplicate and don’t over-communicate either, keep it simple
- Be repetitive in what you want
- Keep communication short and precise
- Work with deadlines when you’re asking for something, I.e. tomorrow by 12pm
- This is about your Mom and nobody else and you are her best advocate
- Quality of life is a subjective and not an objective measure
- Don’t take no for an answer
- Clinical
- All vital signs are stable on the monitor images you sent
- CO2 is elevated but I would want to see the CO2 in an ABG (Arterial Blood Gas) to verify the number on the screen, as sometimes the numbers on the screen and in the ABG don’t correlate
- Your mother is breathing in PSV-CPAP which is spontaneous ventilation mode, therefore she’s breathing with minimal support
- Why is she drowsy? Because of high co2 (carbon dioxide) or because they are giving her sedation? High CO2 can also come from too much sedation.
- Has there been anything else happening clinically in the last few days that they haven’t shared with you?
- Ask for medical records with deadline
- If they keep persisting with end of life talk a) ask for their hospital or ICU policy about end of life to find out if they are acting according to it. Chances are they are not b) keep repeating what you want c) ask them to stop talking about end of life in front of your mother, that’s highly inappropriate
- Why no cardiologist and no respiratory physician?
- Getting back to mobilisation
- No talk about DNR/NFR> avoid and ignore
- You are your mother’s voice and you just keep advocating for her for her wishes
- General:
- ICU has a shortage of beds, therefore they want to withdraw treatment
- One day in ICU is about 3,000-4,000 Euro per bed day or the equivalent in British pounds or $5,000
- Your mother’s stay is too expensive for them and that’s why they push for end of life
- Keep reminding them of those things and address the elephant in the room

Happy to talk to the consultant or nurse tomorrow.
Keep it simple and take the pressure off you. Nobody can force you to make any decisions. There are no laws around it. You can handle it, I know you can.
You’d be surprised what’ll happen when you put the pressure back on to them.
Wishing you and your family all the best for now.
Kind Regards
Patrik
Related articles and Recommended Information:
Dear Patrik,
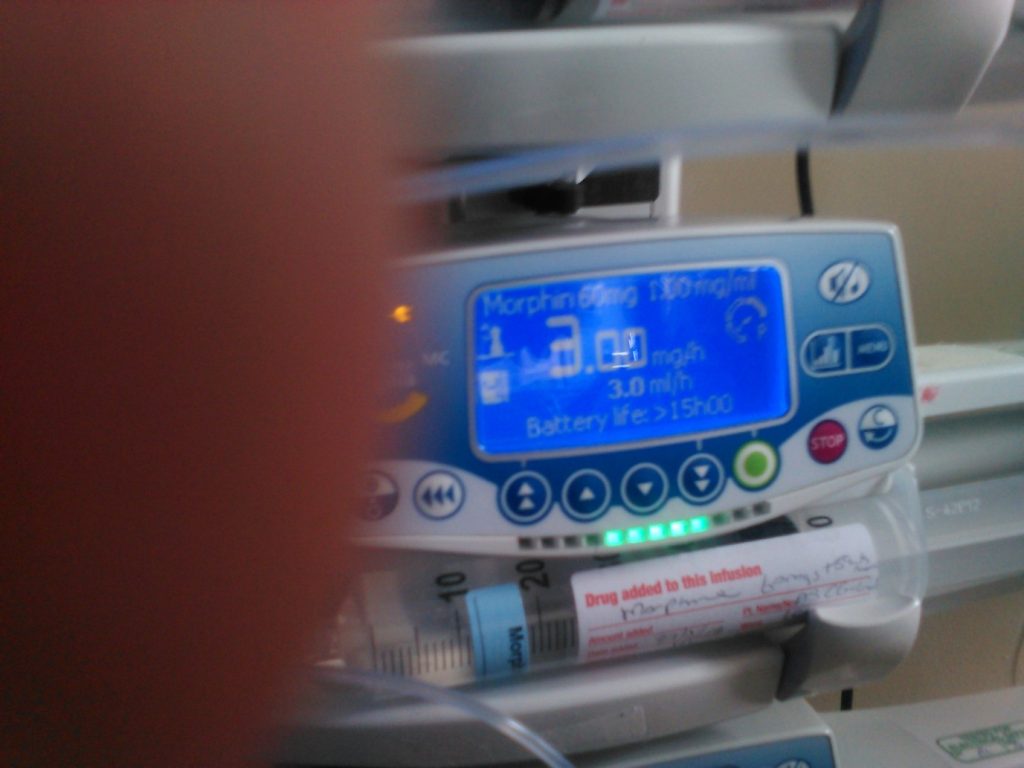
Some Images attached from today.
Including Morphine dose 3 and (I think) insulin at dose 2. Insulin stopped later in day. new med added later in day and Morphine up to 4. Morphine only started today – I think this morning.

Hi Richard,
The Morphine concerns me.
Why is she getting Morphine?
Morphine is only going to make her drowsy and potentially “prepare” for end of life.
Unless she has been in serious pain and discomfort there is no reason to give Morphine.
Morphine will sedate her and make her drowsy. One of the major side effects of Morphine is respiratory depression. Whilst your Mum is still breathing spontaneously, her CO2 is around 65 mmHG (normal is 35-45) and the Morphine is not going to help to bring it down.
I understand your Mum has COPD and therefore her baseline CO2 would be higher than normal, but 65 mmHg is still too high even with a higher than usual baseline!
If she’s getting more and more drowsy because of the Morphine, CO2 will increase and they would need to change ventilation settings to get it down. A high CO2 will also make her even more drowsy.
Morphine is one of the drugs when Patients are being euthanised. Unless they have a clear explanation why they are giving the Morphine they should be stopping it, so your Mum can wake up and participate in any decision making going forward.
Vital signs stable besides the PCO2 but blood pressure a bit low.
Kind Regards
Patrik
Recommended information about DNR:
Hi Patrik,
2 attachments – one from me and one from Heather.
Draft – done quickly rough and ready – covers many of main points.
Written late last night, so excuse bit direct and blunt what I said in meeting etc – I was polite, spoke less, did not agree to anything, but did my best to push for information and seek clarity and patient centred etc. Explained that I was concerned about communication issues etc.
– I have tried to be as accurate as possible but written from memory and medical details might be slightly approximate with strive to understand what being said and work it out as lay person.
Hope helps. Will fill in details with you later if needed – feel free to ask details/clarity etc.
Thanks,
Richard
Here are the meeting notes from Heather
Old notes off your mums file – previous blood clot on lungs.
Cardiac Failure (Heart Failure) by 1
COPD but no follow up
passing little urine
weak
was in pain/stiffness of joints
blood gases deteriorating in last couple of days
Infection in lungs (Pneumonia) again
is getting fluids in but not coming out other end causing swelling to arms & legs
saying cells/vessels leaking/valves
sign of end are near
all of above only started since they talked to her behind our backs
palliative care called in no End-of-Life/Palliative care policy yet except on meds.
They know there are national guidelines but only at committee stage in hospital
Dr Smolensk – no withdrawal of ventilator – there should be no change in her medical care.
palliative just add on i.e. sedation and painkilling morphine
they had given her full notes to palliative care but not us
mentioned re lung cardio urologist specialists not in hospital – their attitude was that ICU had general consultants good enough!!
(Not complete but due to haste to send out – covers much of the meeting)
Recommended:
Here are my meeting notes
- Attendance: Dr Smolensk – Senior Anesthesiast, Palliative Doctor, Patient Nurse, Ward Nurse, Manager, Heather (cousin of Patient) Margaret (aunt of patient), Richard (son and next of kin).
- Initial intro by Dr Smolenks – Mum arrived with respiratory issues, cardiac arrest, heart failure, kidney issues and lung condition (did not specify COPD but fibrous I think). I mentioned COPD and queried this re diagnosis and treatment of COPD etc. No real information in response except it was in her file and that infection had further reduced lung function.
- The nurse’s feedback that they felt mum had significantly weakened and they were very worried about her.
- Palliative consultant feedback re swollen arms/legs and stiffness of arms/general discomfort.
- Key new information re urine output much reduced today. Suggesting includes liquids intake but not coming out via kidneys as urine – vessels breaking down causing swelling in arms and legs -a bad sign. Said they are unable with meds. to get balance right for all organ systems?
– Asked about drowsiness and cause. No clear response to this, just said she was much weaker. I asked if any medication changes. No clear answer to this. I then asked about CO2 output etc., They seemed to say this was pretty good at moment.
– Also (think from memory) they seemed to indicate blood pressure had been ok but not sure now. Referred to blood gas decline but no details given. Maybe later images from day (to be shared) will show more. Will check with Heather in morning.
Recommended:
- I did ask for:
a) End of life policy guidelines.
- Palliative care gave evasive and rather vague answer along lines that they were working on this in sections and what exactly/which part was I needing to see… I think they do not have these guidelines (apart from maybe core medicine part) and are gradually compiling this. I did express surprise and concern, they did not have these available for anyone in ICU/hospital. (Heather may be able to explain this better).
- From Heather: national end of life policy but hospital only at committee stage and have only agreed/implemented the medication section
b) Mum patient notes to be provided by 3pm next day- Ward Nurse said she did not have authority to provide these and would need to refer to others – I think the Records office possibly, I asked her to follow this up for me. I was not convinced she will do this but I did politely ask for this very clearly and firmly that I wanted to have these. (I will do my best to follow this up. Submit main form to records office and ask again).
c) I made it clear that I was most unhappy that important discussions about Mum’s wishes re wish to live etc. had taken place with no family support or consultation over about last three days – I felt not helpful, could make patient feel pressured, lack of support, scope for misunderstanding of wishes etc. – so not ‘patient centred’ in terms of support and not good practice etc. Noted her inability to speak etc. I made it very clear that I did not want this to happen again and sought their agreement on this – very hard to be sure they were agreeing but no-one refused or objected, (disappointed no-one seemed to be troubled at all – but this was my perception, so perhaps some were noting and will respect feedback/wishes).
- I brought up topic of speech support and use of valve and that I understood that it could be used before ventilation ceased. [So their comment about not to consider this ‘until later’ – ventilation support ended, some inconsistency, not clear or helpful.] Esp. in light of key discussion with her over last few days.
- Discussed meeting/discussion tomorrow include our nurse consultant, to assist us, who has ICU background. They agreed. Dr Smolensk to be involved if possible for this (his day off but around and he said, he would make himself available).
Additional:
- Early in meeting, Heather did bring up topic of lack of any specialist diagnosis for Mum re lungs, heart, kidneys etc. and they confirmed not available at hospital etc, said they were ok and doing fine for patients with provision including general consultants… (approximate version of explanation/justification)
- Margaret very upset near end of meeting ( re Mum – (her sister) – connect with Mum believing she is so ill and possible could be
Richard
Recommended and additional information:
Hi Richard,
Thank you for your reports.
ABG’s deteriorating could be sign of infection, we can discuss later.
I’ve seen your latest images.
They have now changed the ventilation settings and she’s not breathing spontaneously any longer. The machine is doing most of the work.
Probably a side effect of the Morphine. CO2 still high. They could bring it down by increasing her breaths per minute or by increasing the pressure support and by potentially ceasing Morphine. It looks like she’s on 4 of Morphine but the image with the infusion is not quite clear. The infusion with 2 was Insulin yesterday unless they have ceased it, it might still be Insulin.
Doctor talking rubbish if he says ventilation shouldn’t be withdrawn whilst he’s increasing Morphine. The Morphine will eventually kill her if they don’t stop it, especially if kidneys are starting to fail.
They are basically trying to euthanise your Mum by telling you they continue medical treatment but put her to sleep on the other end with Morphine.
We can talk about this in more details when we get on the phone.
Will be busy but ready and available when you need me.
Here are my comments on your report in red below.
> Some thoughts and questions. If COPD or lung fibrosis is one of the main issues, they must have done a baseline CO2 test on admission. What was it and how does it compare with her current CO2 levels?
Given the CO2 levels on the monitor (~65 mmHG) and with yesterday’s ventilation settings PSV/CPAP I question that CO2 has gone down, especially with the commencement of a Morphine infusion.
Morphine has respiratory depression as a major side effect, hence why they now put her in a controlled ventilation mode(PRVC) where she stopped breathing by herself and gets 10 breaths/minute delivered by the machine.
In order to get the CO2 down the respiratory rate would have to be increased and Morphine would have to be reduced or ceased altogether.
Another feature that could be used to reduce CO2 is to increase pressure support on the ventilator. I couldn’t see that either.
The fact of the matter is that a high CO2 and a Morphine infusion combined would make your mom drowsy and unable to participate in any decisions making.
Unless there was severe pain, there shouldn’t have been any reason to start Morphine besides “preparing” for an end of life situation.
- The nurse’s feedback that they felt mum had significantly weakened and they were very worried about her.
> If she has weakened, why Morphine? It’s making her even weaker
- Palliative consultant feedback re swollen arms/legs and stiffness of arms/general discomfort.
- Key new information re urine output much reduced today. Suggesting includes liquids intake but not coming out via kidneys as urine – vessels breaking own causing swelling in arms and legs -a bad sign. Said they are unable with meds. to get balance right for all organ systems?
> If kidneys are failing and the doctors are saying she is for full treatment, has dialysis been considered as an option?
> It’s much easier to get the balance right with dialysis
- Asked about drowsiness and cause. No clear response to this, just said she was much weaker. I asked if any medication changes. No clear answer to this. I then asked about CO2 output etc., They seemed to say this was pretty good at moment.
> As far as I can see the drowsiness is a combination of high CO2 and Morphine
> Potentially also infection. Have they found a source of infection?
- Also (think from memory) they seemed to indicate blood pressure had been ok but not sure now. Referred to blood gas decline but no details given. Maybe later images from day (to be shared) will show more. Will check with Heather in morning.
> If BP has gone down has she been commenced on inotropes/vasopressors like Noradrenaline, Adrenaline?
> Inotropes/vasopressors are considered life support and again, if she is for full treatment they should have started it
> Furthermore, with low BP the kidneys would suffer even more, due to no kidney perfusion from low blood pressure, hence the need for inotropes/vasopressors
> More about inotropes/vasopressors here
> http://intensivecarehotline.com/your-loved-ones-treatment/inotropes/
> Blood gas has probably declined for the reasons I mentioned before. Also, her Oxygen saturation is only 89% in the screen shot. It should be 92% and above. She’s only on 30% of oxygen and that could be increased with no problems to get o2 saturation >92%
More information and recommended article behind the ICU:
- I did ask for:
a) End of life policy guidelines.
- Palliative care gave evasive rather vague answer along lines that they were working on this in sections and what exactly/which part was I needing to see… I think they do not have these guidelines (apart from maybe core medicine part) and are gradually compiling this. I did express surprise and concern, they did not have these available for anyone in ICU/hospital. (Heather may be able to explain this better).
- From Heather: national End-of-Life policy but hospital only at committee stage and have only agreed/implemented the medication section
> keep asking to keep the pressure on
b) Mum patient notes to be provided by 3pm next day- Ward Nurse said she did not have authority to provide these and would need to refer to others – I think the Records office possibly, I asked her to follow this up for me. I was not convinced she will do this but I did politely ask for this very clearly and firmly that I wanted to have these. (I will do my best to follow this up. Submit main form to records office and ask again).
> keep asking to keep the pressure on
c) I made it clear that I was most unhappy that important discussions about Mum’s wishes re wish to live etc. had taken place with no family support or consultation over about last three days – I felt not helpful, could make patient feel pressured, lack of support, scope for misunderstanding of wishes etc. – so not ‘patient centred’ in terms of support and not good practice etc. Noted her inability to speak etc. I made it very clear that I did not want this to happen again and sought their agreement on this – very hard to be sure they were agreeing but no-one refused or objected, (disappointed no-one seemed to be troubled at all – but this was my perception, so perhaps some were noting and will respect feedback/wishes).
> keep asking to keep the pressure on and get agreement
> as far as I can see, the Morphine and the high CO2 that could have been managed earlier in the week by changing ventilation settings could have made her more awake to participate in any decision making
- I brought up topic of speech support and use of valve and that I understood that it could be used before ventilation ceased. [So their comment about not to consider this ‘until later’ – ventilation support ended, some inconsistency, not clear or helpful.] Esp. in light of key discussion with her over last few days.
- Discussed meeting/discussion tomorrow include our nurse consultant, to assist us, who has ICU background. They agreed. Dr Smolensk to be involved if possible for this (his day off but around and he said, he would make himself available).
Recommended:
Additional:
- Early in meeting, Heather did bring up topic of lack of any specialist diagnosis for Mum re lungs, heart, kidneys etc. and they confirmed not available at hospital etc, said they were ok and doing fine for patients with provision including general consultants… (approximate version of explanation/justification)
> Ask them what they mean by “doing fine”. Ask them for their mortality rate. Survival rates in ICU are 90%-93% of all Patients, why should your Mom be in the 7%-10% bracket?
> Lack of speciality input such as cardiologist, respiratory physician, nephrologist
Here are my thoughts and comments in red for Heather’s meeting report
Old notes off your mums file – previous blood clot on lungs.
cardiac failure by 1
copd but no follow up
> especially with chronic COPD it would have definitely required specialist input from a respiratory physician
passing little urine
> Again, why no Dialysis if she is for “full medical treatment”. This would include Dialysis if the kidneys are failing and can’t be managed by medication
Weak
> Weakness can happen after 4 weeks in ICU, she’s allowed to be weak after such a long time in ICU
was in pain/stiffness of joints
> In order to manage stiffness, she needs to be mobilised or at leats have regular Physiotherapy
blood gases deteriorating in last couple of days
> Why did they deteriorate?
> My first thoughts are that she was in a spontaneous ventilation mode with minimal support. That’s fine for somebody who is weaning off the ventilator. It also means she was close(r) to coming off the ventilator. What happened in order for the ABG’s to deteriorate
> Is she having a Pneumonia or chest infection
> Is she still having daily chest x-rays?
> How often does she need tracheostomy suctioning?
Recommended information about tracheostomy:
infection again
> Where is the infection?
> Have they started looking for sources?
> e. tested chest secretions, urine and blood to screen for infection(s)?
is getting fluids in but not coming out other end causing swelling to arms & legs
saying cells/vessels leaking/valves
> If the vessels are “leaking” she might have a significant deficit in Albumin levels. Have they checked her Albumin levels and if they are low, they should consider to replace Albumin to stop the vessels from leaking?
> Replacing Albumin could also increase her blood pressure without the need for inotropes/vasopressors
sign of end near
> If signs for end are near, how did she get there?
> Potentially through unmanaged high CO2 and commencement of Morphine. Both make Patients very drowsy
all of above only started since they talked to her behind our backs
palliative care called in no End-of-Life/Palliative care policy yet except on meds.
know there are national guidelines but only at committee stage in hospital
Dr Smolensk – no withdrawal of ventilator – there should be no change in her medical care.
> There should be escalation of treatment as long as there is no DNR or any other mutually agreed withdrawal of treatment plans
palliative just add on i.e. sedation and painkilling morphine
> This could be considered euthanasia
Let me know when you want to get on the phone again, I can be available any time.
Kind Regards
Patrik
Stay tuned for more episodes with Richard next week!
How can you become the best advocate for your critically ill loved one, make informed decisions, get peace of mind, control, power and influence quickly, whilst your loved one is critically ill in Intensive Care?
You get to that all important feeling of making informed decisions, get PEACE OF MIND, CONTROL, POWER AND INFLUENCE when you download your FREE “INSTANT IMPACT” report NOW by entering your email below!
In Your FREE “INSTANT IMPACT” report you’ll learn quickly how to make informed decisions, get PEACE OF MIND, real power and real control and how you can influence decision making fast, whilst your loved one is critically ill in Intensive Care! Your FREE “INSTANT IMPACT” Report gives you in-depth insight that you must know whilst your loved one is critically ill or is even dying in Intensive Care!
Sign up and download your FREE “INSTANT IMPACT” REPORT now by entering your email below! In your FREE “INSTANT IMPACT” REPORT you’ll learn how to speak the “secret” Intensive Care language so that the doctors and the nurses know straight away that you are an insider and that you know and understand what’s really happening in Intensive Care! In your FREE report you’ll also discover
- How to ask the doctors and the nurses the right questions
- Discover the many competing interests in Intensive Care and how your critically ill loved one’s treatment may depend on those competing interests
- How to eliminate fear, frustration, stress, struggle and vulnerability even if your loved one is dying
- 5 mind blowing tips& strategies helping you to get on the right path to making informed decisions, get PEACE OF MIND, control, power and influence in your situation
- You’ll get real world examples that you can easily adapt to your and your critically ill loved one’s situation
- How to stop being intimidated by the Intensive Care team and how you will be seen as equals
- You’ll get crucial ‘behind the scenes’ insight so that you know and understand what is really happening in Intensive Care
- How you need to manage doctors and nurses in Intensive Care (it’s not what you think)
Thank you for tuning into this week’s YOUR QUESTIONS ANSWERED episode and I’ll see you again in another update next week!
Make sure you also check out our “blog” section for more tips and strategies or send me an email to [email protected] with your questions!
Also, have a look at our membership site INTENSIVECARESUPPORT.ORG for families of critically ill Patients in Intensive Care here.
Or you can call us! Find phone numbers on our contact tab.
Also check out our Ebook section where you get more Ebooks, Videos and Audio recordings and where you can also get 1:1 counselling/consulting with me via Skype, over the phone or via email by clicking on the products tab!
This is Patrik Hutzel from INTENSIVECAREHOTLINE.COM and I’ll see you again next week with another update!
Related Articles:
- 5 Ways to have control, power and influence while your loved one is critically ill in Intensive Care
Related Articles:
 Is it best for my Dad to go from ICU to step-down or should he be going to Rehabilitation straight away?
Is it best for my Dad to go from ICU to step-down or should he be going to Rehabilitation straight away?
 The ICU team is telling me and my mom to stop her medical treatment. Can they end her life without my consent?
The ICU team is telling me and my mom to stop her medical treatment. Can they end her life without my consent?
 The ICU team is giving my mom too many sedatives. Are they slowly killing her or are they helping her to wean off the ventilator?
The ICU team is giving my mom too many sedatives. Are they slowly killing her or are they helping her to wean off the ventilator?
 What are the chances of survival after a tracheostomy?
What are the chances of survival after a tracheostomy?
 I don’t think the ICU wants to help my mother to fully recover and get off the ventilator. How can I find out?
I don’t think the ICU wants to help my mother to fully recover and get off the ventilator. How can I find out?