


Hi, it’s Patrik Hutzel from INTENSIVECAREHOTLINE.COM where we instantly improve the lives for Families of critically ill Patients in Intensive Care, so that you can make informed decisions, have PEACE OF MIND, real power, real control and so that you can influence decision making fast, even if you’re not a doctor or a nurse in Intensive Care!
This is another episode of “YOUR QUESTIONS ANSWERED” and in last week’s episode I answered another question from our readers and the question was
You can check out last week’s question by clicking on the link here.
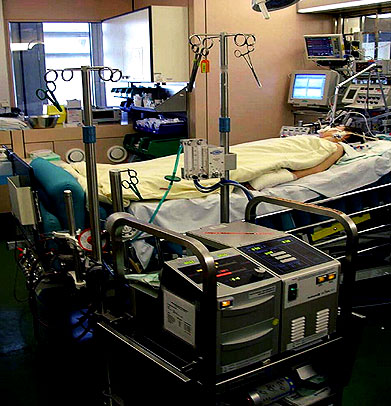
In this episode of “YOUR QUESTIONS ANSWERED” I want to answer a question from one of my clients Ernie as part of my 1:1 consulting and advocacy service! Ernie’s dad is in ICU with pancreatitis and Ernie is asking when can the ICU Team wean his dad off the ventilator.
My Dad is in ICU with Pancreatitis. When Can They Wean My Dad Off the Ventilator?
Patrik: Intensive Care Hotline, Patrik speaking, how can I help?
Ernie: Hi Patrik. This is Ernie.
Patrik: Yes. Thank you, Ernie, for getting back to me, I’ve been on the phone to Connie and she asked me to keep you a quick summary.
Ernie: Ok. So, what’s the information about?
Patrik: So, we had a good chat. So the overall condition is still fairly grave. I wouldn’t say great, but certainly critical. The main issue is still the pancreas. The pancreas is still inflamed. He has pancreatitis. The pancreas markers in the blood are still elevated. The main issue they are dealing with.
RECOMMENDED:
Ernie: Are there any other issues?
Patrik: There are three main issues. Number one, the pancreas, number two he’s still got fluids on his chest and the chest infection. And number three, which sounds new to me is, he’s got an ileus, have you heard of an ileus? Basically a bowel obstruction, which is concerning to me. It’s probably one of the complications that often comes up when someone is in an induced coma because there’s reduced bowel activity.
Ernie: Yes, that’s definitely concerning. Can you tell me more about it?
Patrik: So, he is sort of opening his bowels a little bit and they’re treating it with medication with laxatives and also, something that is trying to increase the peristaltic of the bowels. Because of him not opening his bowels for the last two days, there is a lot of pressure pushing on his lungs because he’s tummy is so tender, so tight, you know, so there’s a lot of pressure pushing on his lungs because of that which means his lungs can’t really expand, which increased his oxygen demand.
Ernie: Oh, I see.
Patrik: He’s on 55% of oxygen on the ventilator. Now room air is 21%, the air that you and I breathe is 21%. So he’s on 55% of oxygen and therefore, they can’t wean him off the ventilator yet, which is understandable. I mean, as soon as his oxygen requirements are going down, they can also then start weaning off the ventilator.
Patrik: But as soon, you know, at the moment, that’s not an option, which means they can’t take him out of the induced coma yet and highlighting just what I mentioned to you in our initial discussion that, the longer the induced coma goes on and ventilation, there are those risks that we talked about in terms of deconditioning muscle atrophy.
Ernie: Yes, I remember what we discussed about that.
Patrik: And then when someone does come out of an induced coma, eventually issues of confusion, potentially a psychosis, you know, short term psychosis, delirium, all of that. So they are fully aware of those risks. So from that perspective, they would like to wean him off the ventilator as quickly as possible, but obviously at the moment with the bowel issue, they’re dealing with another issue on top of that.
Recommended:
Ernie: Ok.
Patrik: They are definitely trying to get on top of that. Giving him what we talked about, the appearance of the laxative, as well as the medication that’s increasing the peristaltic of his bowels, but you know, again, it’s probably a bit of a catch 22 because even though they’re doing that, yes it’s very uncomfortable for him. I would imagine his bowels or his tummy is so swollen, so distended, they’re giving medication to increase the peristaltic of his bowels.
Ernie: So they need to give my brother more sedation to help ease the discomfort at least.
Patrik: Yes, potentially increasing the need for sedation and pain medication because of the discomfort, you know, it’s sort of a catch 22 almost.
Ernie: Have they told any other clinical info?
Patrik: So they’ve done a CT scan, head to toe. Like they said the fluids on his lungs that they don’t need to drain yet. They said there is the risk that they may need to drain the fluids on the lungs.
Ernie: Ok.
Patrik: They are also waiting for blood cultures to come back to see whether the fluid accumulation on the chest is also an infection. So at the moment, they’re treating him with broad spectrum antibiotics, which is, you know, it’s not quite defined what they’re treating yet, but that’s what they’re waiting for.
Ernie: Alright. So if there will be a result for the blood culture, what will happen next?
Patrik: Once they’ve got the results, they can use a very targeted antibiotic, which hopefully will help with the infection. Right. News is that all other organs are stable. Hardly stable. His brain is intact. The kidneys are working and he’s not on any other mechanisms of life support.
Ernie: Good to hear that. But will the infection later on will have an effect to his overall condition?
Patrik: What sometimes happens is when someone has an infection and they’re on sedation, their blood pressure often goes down to dangerous levels. And if that’s the case, they end up on what’s called inotropes/vasopressors, which is an artificial, blood pressure medication to increase blood pressure. They don’t need that at the moment, which is a good sign, which means the heart is strong enough.
Ernie: Ok. How about his kidneys?
Patrik: The kidneys seem to work, so we’re really dealing with mainly chest issues, pancreas, obviously, as well as, the bowels, right. I then asked about the tracheostomy. They said it’s too early to look into that. Obviously they did say that, like we talked about earlier, if it comes to sort of stay 14 days on a ventilator that a tracheostomy is something they would consider.
Suggested articles:
Ernie: Alright. I hope it can be avoided.
Patrik: Look. There’s nothing in there that I believe can’t be overcome. You know, things like, I asked about blood results, things like the white cell count, the white cell count in the blood is the main marker for an infection that is actually coming down slowly, which is a good sign. So it looks like they’re doing all the right things, but the bowel obstruction is certainly something that I don’t like.
Patrik: Because I’ve seen this many, many times, and it’s certainly something that could cause a delay with coming off the ventilator. It’s often very painful from what I’ve seen and hopefully they will get the bowels going in the next few days because the worst case scenario in a situation like that, if they can’t get the bowels going is that, they would have to perform surgery eventually and would prolong the coma.
Ernie: It would just not be a good thing. I hope they can get the bowels going.
Patrik: I have a very high level of confidence there. I also found the doctor to be very friendly, not evasive of any questions, not defensive, sometimes that’s a very good sign. You know, they can be very defensive. They can be very negative. I didn’t have that feeling at all. No, no, definitely.
Ernie: That’s a good sign indeed.
Patrik: Definitely. The other good thing that he said was the pancreas is not necrotic, which means the tissue of the pancreas is intact.
Ernie: Ok, I get that. How about the feeding? Have they been feeding my brother?
Patrik: Yes, the other thing they are doing now as well is they’re very gently starting to feed him. We’ve been said, they are using the nasal gastric tube to give him like 10 mls an hour of feeds which is a good sign as well.
Ernie: What is that again? Nasal gastric feeds?
Patrik: Yeah, just some nasal gastric feeds. Basically it feeds that that’s going into his stomach, but it’s a very low dose. It’s like 10 meals an hour, which is nothing really.
Ernie: Alright.
Patrik: But that they need to do to sort of probably get the bowels going from the top as well, slowly. So it looks to me like they’re covering all their basis. Their biggest concern or one of their biggest concerns at the moment is that if they’re not finding the source of infection that he could end up with sepsis, have you heard of the term sepsis, right?
Ernie: Sepsis is an infection right?
Patrik: Yeah. That’s right. It would been an infection in the blood. So, which is why they’re waiting for the results and then potentially..
Ernie: So they can give my brother the targeted antibiotic to help him with the infection.
Patrik: Correct. Correct.
Patrik: So with all that being said, what would you say that’s an improvement from your last update? Is it a deterioration? What do you think?
Ernie: I think, there’s improvement.
Patrik: Right. Yes. And you can see how all systems need to work together to get him out of this.
Ernie: Yes, you’re right.
Patrik: The other thing is because you asked earlier about tracheostomy to me. I can tell you that. Let’s just say, hypothetically, he was day 14 today, right? Hypothetically, if he was to have a tracheostomy, now they could reduce his sedation straight away because the tracheostomy is so much more comfortable to tolerate compared to the breathing tube.
Suggested articles:
Patrik: So a tracheostomy has the advantage of that. It’s more or less painless once it’s there. Whereas with the breathing tube, you got to put someone in an induced coma because it’s so uncomfortable. Have you seen the breathing tube?
Ernie: Yes, the tube inside his mouth.
Patrik: Right, right. So it’s so uncomfortable. It’s basically a tube in your throat, right? I mean, can’t get more uncomfortable than this. So, you know, the, the advantage of a tracheostomy is simply, it’s much more comfortable. You can pretty much take off sedation straight away because it’s so much easier to tolerate.
Ernie: Ok, that is the advantage.
Patrik: That’s the advantage in a nutshell.
Ernie: Ok. How about for the disadvantage?
Patrik: The disadvantage is simply, if you can avoid it, it’s good if you can avoid it because it’s a procedure, sort of a mini operation if you will, risk of infection. You know, there’s also, I believe there’s also a tendency in some ICU that once they have a tracheostomy, it sort of, can make people complacent in terms of trying to be weaning a person off the ventilator.
Ernie: Alright.
Patrik: It could be an element of complacency coming in. Whereas now, the goal is to wean him off the ventilator. That’s the goal. Once the tracheostomy is there again, my concern is there could be a sense of complacency kicking in thinking, not from your point of view from, from the treating team’s point of view. But I’m hopeful again.
Ernie: Yes, definitely the goal is to wean my brother off the ventilator.
Recommended:
Patrik: What I can see is definitely working in his favor, you look at average age in ICU of ICU patients, it’s fairly high, 46, he would be one of the youngest ones in there, and that’s certainly working in his favor I believe.
Ernie: Yes, I think so too.
Patrik: The other thing that I asked is about COVID. They’ve tested him quite a few times, so that’s all negative because especially with lung failure or anybody that’s ventilated, the first thing in my mind at the moment is, Oh, what about COVID?
Ernie: Ok.
Patrik: So, that is something that needs to be ruled out, especially in the current environment.
Ernie: Yes, that’s right.
Patrik: Yeah. So, look, it’s from a bigger picture perspective, Ernie, as well, in ICU, it’s often two steps forward, one step back and, you know, it’s often like a marathon and not a sprint. And, I believe at the moment the bowel issue needs to be sorted and once that’s sorted, hopefully his ventilation needs are coming down.
Ernie: Yes. I hope so too.
Patrik: That would be so important. And also once the pressure is off the bowels, the pressure will also be off the pancreas. It’s all one, you know, it’s all one system really.
Ernie: Alright.
Patrik: I tell you what I would like to say, it’s very easy to get impatient in a situation like that. There’s eight days in ICU. It’s been probably a hell of a trip for you and your family. Again, in the biggest scheme of things, eight days in ICU is not a long time. I would argue that with the condition today, he’ll be in it at least for another eight days. And then what is really important in a situation like that is, you mustn’t give up hope, never, never give up hope. You know, and because there could be another, there can be setbacks in a situation like that.
Recommended articles:
Ernie: My hopes are all high.
Patrik: That’s good to know.
Patrik: I’ll tell you what can also happen down the line. Let’s just say, God forbid, let’s just say it’s not getting better. The ICU will turn negative and they will probably turn negative very quickly if he’s not improving in a timeframe that’s convenient for them. And, let’s just say, God forbid, he’s taking a turn to the worst, they will become negative.
Patrik: So just to be prepared for that, and they will become negative by default, that’s part of their job to manage their downside. So don’t be discouraged by them potentially turning negative. Right. It’s part of their job. It’s part of managing their risk in terms of over promising and under delivering, they can never do that.
Ernie: I see that.
Patrik: They would under promise.
Ernie: Ok. I’ll keep that in mind.
RECOMMENDED:
Patrik: So always, always read between the lines. So just because they might turn negative one day doesn’t mean that there is hope loss. It’s just their communication style around, “how do we manage our downside?”
Ernie: Ok. So, what could be the current problem now for my brother?
Patrik: Yeah. It’s about the whole abdominal tract, really. That’s playing up at the moment and hopefully they can get that under control without causing too much pain for him.
Ernie: Alright. Thank you Patrik for your time. I’ll give you another call next time for updates with regards to my brother’s condition in ICU.
Patrik: Okay. Thank you, Ernie. All the best for now. Thank you. Bye bye.
How can you become the best advocate for your critically ill loved one, make informed decisions, get peace of mind, control, power and influence quickly, whilst your loved one is critically ill in Intensive Care?
You get to that all important feeling of making informed decisions, get PEACE OF MIND, CONTROL, POWER AND INFLUENCE when you download your FREE “INSTANT IMPACT” report NOW by entering your email below!
In Your FREE “INSTANT IMPACT” report you’ll learn quickly how to make informed decisions, get PEACE OF MIND, real power and real control and how you can influence decision making fast, whilst your loved one is critically ill in Intensive Care! Your FREE “INSTANT IMPACT” Report gives you in-depth insight that you must know whilst your loved one is critically ill or is even dying in Intensive Care!
Sign up and download your FREE “INSTANT IMPACT” REPORT now by entering your email below! In your FREE “INSTANT IMPACT” REPORT you’ll learn how to speak the “secret” Intensive Care language so that the doctors and the nurses know straight away that you are an insider and that you know and understand what’s really happening in Intensive Care! In your FREE report you’ll also discover
- How to ask the doctors and the nurses the right questions
- Discover the many competing interests in Intensive Care and how your critically ill loved one’s treatment may depend on those competing interests
- How to Eliminate fear, frustration, stress, struggle and vulnerability even if your loved one is dying
- 5 mind blowing tips & strategies helping you to get on the right path to making informed decisions, get PEACE OF MIND, control, power and influence in your situation
- You’ll get real world examples that you can easily adapt to you and your critically ill loved one’s situation
- How to stop being intimidated by the Intensive Care team and how you will be seen as equals
- You’ll get crucial ‘behind the scenes’ insight so that you know and understand what is really happening in Intensive Care
- How you need to manage doctors and nurses in Intensive Care (it’s not what you think)
Thank you for tuning into this week’s YOUR QUESTIONS ANSWERED episode and I’ll see you again in another update next week!
Make sure you also check out our “blog” section for more tips and strategies or send me an email to [email protected] with your questions!
Also, have a look at our membership site INTENSIVECARESUPPORT.ORG for families of critically ill Patients in Intensive Care here.
Or you can call us! Find phone numbers on our contact tab.
Also check out our Ebook section where you get more Ebooks, Videos and Audio recordings and where you can also get 1:1 counselling/consulting with me via Skype, over the phone or via email by clicking on the products tab!
This is Patrik Hutzel from INTENSIVECAREHOTLINE.COM and I’ll see you again next week with another update!
Related Articles:
- 5 Ways to have control, power and influence while your loved one is critically ill in Intensive Care
Related Articles:
 The ICU is telling me that my father’s condition is hopeless. Should I stop his medical treatment?
The ICU is telling me that my father’s condition is hopeless. Should I stop his medical treatment?
 My Brother is Ventilated in ICU with Pneumonia and the ICU team Issued a DNR (Do Not Resuscitate) Status for Him Without My Consent? What Should I Do?
My Brother is Ventilated in ICU with Pneumonia and the ICU team Issued a DNR (Do Not Resuscitate) Status for Him Without My Consent? What Should I Do?
 Why COVID-19 Can Make Someone Critically Ill
Why COVID-19 Can Make Someone Critically Ill
 Is it Safe for My Brother to Get Out of ICU Quickly Once He’s Off the Ventilator?
Is it Safe for My Brother to Get Out of ICU Quickly Once He’s Off the Ventilator?
 My Dad Is In ICU And Still Vulnerable But Why Is The ICU Team Rushing My Dad to be Transferred to the Ward?
My Dad Is In ICU And Still Vulnerable But Why Is The ICU Team Rushing My Dad to be Transferred to the Ward?