


Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS
Hi, it’s Patrik Hutzel from INTENSIVECAREHOTLINE.COM where we instantly improve the lives for Families of critically ill Patients in Intensive Care, so that you can make informed decisions, have PEACE OF MIND, real power, real control and so that you can influence decision making fast, even if you’re not a doctor or a nurse in Intensive Care!
This is another episode of “YOUR QUESTIONS ANSWERED“ and in last week’s episode I answered another question from our readers and the question last week was
You can check out the answer to last week’s question by clicking on the link here.
In this week’s episode of “YOUR QUESTIONS ANSWERED“, I want to answer another question from one of our readers and the question this week is
My 57 year old Dad has been in Intensive Care with Cardiomyopathy and Pneumonia for 5 weeks! He’s still in an induced coma and still doesn’t have a tracheostomy, HELP! (PART 2)
This series of questions from Garry are excerpts from numerous 1:1 phone and email counselling and consulting sessions with me over a two month period.
Garry and his family went through many challenges while his Dad was in Intensive Care and I felt very privileged helping Garry through this difficult time in his and his Dad’s life!
Garry writes
Hi Patrik,
after our last phone call on Friday I’ve gotten back to the ICU doctors and demanded a tracheostomy.
Thank you for explaining to me that they have misled me and most of all my Dad and that it was inappropriate to not have my Dad get a tracheostomy for nearly 5 weeks!
I’ve pretty much explained all to them what you and I discussed on our last call that he needs the tracheostomy ASAP and that he needs to get out of the induced coma ASAP!
At first they were telling me that they can’t do it and that they have to call in a specialist from another hospital and that it couldn’t be done before mid next week, but after me mentioning that I’d be looking to transfer my Dad to another hospital they’ve done the tracheostomy on Sunday, mid-afternoon. All went ok with no complications.
However he is still heavily sedated. For the past few days he has been having “unstable” episodes with his heart. So they had to increase the inotropes (Dobutamine) in order to stabilize him.
I asked about reducing the sedation and they have said that they tried after the tracheostomy but he wasn’t “triggering” the ventilator and he was becoming agitated so they had to re-sedate him.
They plan to start reducing the sedation again tomorrow.
Here are my most burning questions for now.
- What should I expect to happen from this point forward, now that he has a tracheostomy done?
- Is it right to keep him sedated still at this point?
- They had mentioned that his heart has “decreased” in size, yet he is still having unstable episodes, why might that be?
- How long could this go on for, i.e. how long can he remain on the vent via tracheostomy?
- He still has a build-up of fluids (edema?) – How could this be treated?
- His liver, while not majorly affected, is still showing some signs of being affected, presumably this is all due to the cardiomyopathy (as you said before) and there isn’t anything we can do to treat that other than treat the cardiomyopathy?
- What questions should I now be asking?
That’s all for now
Garry
Hi Garry,
well done for putting things into practice so quickly!
The best work we can do for our clients is when they follow our advice and put our advice into practice! It also shows that our advice works and delivers results.
It’s just a matter of pushing back on them and not take “no” for an answer!
The best advice that I can give someone in a situation like yours is to be “difficult and demanding”!
Related article/video:
I still have huge concerns that your Dad is in a 3 bed ICU and again leaving your Dad in an induced coma for nearly 5 weeks without even explaining to you why he needs a tracheostomy screams negligence to me.
They just don’t have the experience that a bigger ICU has because your Dad’s situation is too complex and complicated to be looked after in such a small ICU. But I will come to that later in more detail.
First, let’s look at your questions in detail. My responses to your questions are in red.
- They’ve done the tracheostomy on Sunday, mid-afternoon. All went ok with no complications. However he is still heavily sedated. For the past few days he has been having “unstable” episodes with his heart. So they had to increase the inotropes. (Dobutamine) in order to stabilise him.
- How are they going to reduce the Dobutamine, what’s their plan?
- If he had unstable episodes of the heart, it’s most likely that he had Ventricular tachycardia, SVT, Atrial fibrillation are the main ones. They can be life threatening> treatable with Adenosin or Amiodarone> quite common in Cardiomyopathy
- Monitoring of Potassium and Magnesium levels and replacement of such when low as it can contribute to unstable episodes
- I asked about reducing the sedation and they have said that they tried after the tracheostomy but he wasn’t “triggering” the vent and was becoming agitated so they had to re sedate him.
- They plan to start reducing the sedation again tomorrow.
- They will most likely need a few attempts to get your Dad out of the induced coma. He’ll be withdrawing from all the sedatives, especially after nearly 5 weeks in an induced coma. They will most likely need to use some medications like Haloperidol, Seroquel or Clonidine to support getting him out of the induced coma. He will be withdrawing from the Midazolam(Versed) he has been having and he will also be withdrawing from the Opiates(=pain relief) such as Morphine or Fentanyl
- As we discussed Garry, 5 weeks in an induced coma to be able to tolerate the breathing tube whilst getting all those powerful and addictive medications such as Midazolam(Versed) and Morphine or Fentanyl screams negligence to me. The minute they realized that they are dealing with such a complex situation they should have
- Referred him to another more specialized Intensive Care Unit
- Done a tracheostomy early on to get him out of the induced coma and minimize the amount of sedation and opiates he’s getting especially in view of a severely weakened heart with the Cardiomyopathy
- Once out of the induced coma, your Dad will most likely go into a state what’s being referred to as ICU Psychosis or ICU delirium. Again, the longer critically ill Patients are kept in an induced coma the higher the likelihood of developing ICU psychosis or ICU delirium from a prolonged induced coma. It’s nothing your Dad or any other critically ill Patient in Intensive Care needs. That’s why it’s so important to get Patients out of an induced coma as quickly as possible and a tracheostomy can help facilitate that.
Here is a link to an article/video around the topic
You may also want to look at those resources:

- What should I expect to happen from this point forward, now that he has a tracheostomy done?
- Get your Dad out of coma ASAP
- Physiotherapy, especially Physiotherapy of the chest to support your Dad to get off the ventilator- My concern is that in a 3 bed ICU they don’t have the experience and the skills to wean somebody off the ventilator
- Potentially weaning trials off the ventilator but it all depends on how effective they can treat the Cardiomyopathy and the Pneumonia
- Is it right to keep him sedated still at this point?
- Not really, but they will have to wake him up slowly as he will be withdrawing from the sedatives and opiates(=pain killers)
- You mentioned that he had unstable episodes with his heart. Again, this could be part of the Cardiomyopathy but it doesn’t help that after 5 weeks induced coma your Dad is most likely having difficulties “waking up” after the induced coma for the reasons I mentioned before.
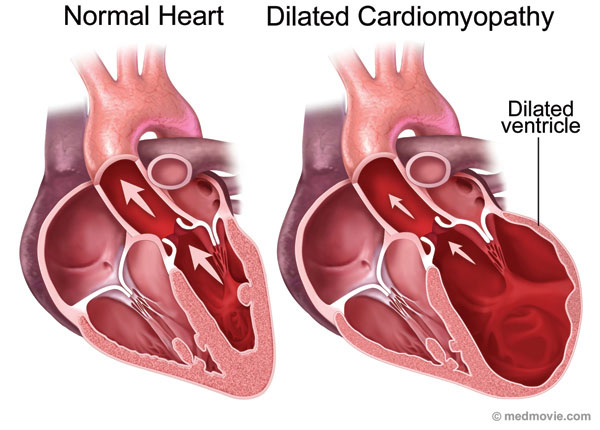
- They had mentioned that his heart has “decreased” in size, yet he is still having unstable episodes, why might that be?
- heart has decreased in size due to Dobutamine and giving Diuretics(Lasix, Frusemide) to increase urine output
- Normally in Cardiomyopathy, the heart increases in size due to the dilatation of the heart because of its reduced ability to pump blood (please see image below). This also increases the risk for stroke as there is a higher chance for a thrombus(=blood clot) to develop. I understand your Dad is on Heparin, therefore at least they are covering or minimizing the risk for a stroke
- The unstable episodes are most likely a result of the Cardiomyopathy. Cardiomyopathy just leaves the heart vulnerable for irregular heart rhythms also known as arrhythmias. It’s also why they are most likely at their wits end already and I’ll come to that later
- How long could this go on for, i.e. how long can he remain on the vent via tracheostomy?
- for many weeks or months, especially with such a prolonged induced coma weakening him. Also, with early treatment for Cardiomyopathy such as ECMO, VAD or even a Heart transplant he could have been tracheostomised and out of the induced coma early on. Again I will explain treatment for Cardiomyopathy on our next call
For now, check out this article/video here
- He still has a build-up of fluids (oedema?) – How could this be treated?
- Mainly with medications also know as Diuretics such as Frusemide and/or Spironolactone to increase Urine output
- It can also be treated with getting your Dad on a Dialysis machine
- Inotropic treatment such as Dobutamine and/or Noradrenaline to increase the contractility of the heart and to increase the blood pressure to maintain adequate kidney perfusion and therefore increased urine output
- Replace Albumin. Especially with your Dad developing liver failure, there is a chance that his Albumin levels in the blood are low. Low Albumin will be causing fluid build up as well
- His liver, while not majorly affected, is still showing some signs of being affected, presumably this is all due to the cardiomyopathy (as you said before) and there isn’t anything we can do to treat that other than treat the cardiomyopathy?
- Liver failure is secondary to cardiomyopathy and secondary to all the sedatives and opiates.
- For now, one of the next steps is to get your Dad off all the sedatives and opiates to reduce the impact on liver and kidneys
- Low cardiac output and poor contractility of the heart with consecutive reduction in reduced liver blood flow is a main causing factor
- The same applies to acute kidney failure in view of poor cardiac output and poor contractility
Here is a link to all the questions from the lady who’s Mum was in ICU for 4 months last year that I consulted. Just to give you an idea that massive challenges can be overcome with the right advice and in the right environment
What questions should I now be asking?
- The questions you should be asking are in view of how to treat the Cardiomyopathy as this is the underlying cause of the liver failing and the kidneys failing
- We will be discussing this on our next call, but my biggest concern is that they have missed the boat already by not making a referral to a more specialized and more experienced ICU who has the know-how and the equipment how to successfully treat the cardiomyopathy
Speak on Wednesday and thanks again for being so proactive, well done!
Take care
Patrik
How can you become the best advocate for your critically ill loved one, make informed decisions, get peace of mind, control, power and influence quickly, whilst your loved one is critically ill in Intensive Care?
You get to that all important feeling of making informed decisions, get PEACE OF MIND, CONTROL, POWER AND INFLUENCE when you download your FREE “INSTANT IMPACT” report NOW by entering your email below!
In Your FREE “INSTANT IMPACT” report you’ll learn quickly how to make informed decisions, get PEACE OF MIND, real power and real control and how you can influence decision making fast, whilst your loved one is critically ill in Intensive Care! Your FREE “INSTANT IMPACT” Report gives you in-depth insight that you must know whilst your loved one is critically ill or is even dying in Intensive Care!
Sign up and download your FREE “INSTANT IMPACT” REPORT now by entering your email below! In your FREE “INSTANT IMPACT” REPORT you’ll learn how to speak the “secret” Intensive Care language so that the doctors and the nurses know straight away that you are an insider and that you know and understand what’s really happening in Intensive Care! In your FREE report you’ll also discover
- How to ask the doctors and the nurses the right questions
- Discover the many competing interests in Intensive Care and how your critically ill loved one’s treatment may depend on those competing interests
- How to eliminate fear, frustration, stress, struggle and vulnerability even if your loved one is dying
- 5 mind blowing tips& strategies helping you to get on the right path to making informed decisions, get PEACE OF MIND, control, power and influence in your situation
- You’ll get real world examples that you can easily adapt to your and your critically ill loved one’s situation
- How to stop being intimidated by the Intensive Care team and how you will be seen as equals
- You’ll get crucial ‘behind the scenes’ insight so that you know and understand what is really happening in Intensive Care
- How you need to manage doctors and nurses in Intensive Care (it’s not what you think)
Thank you for tuning into this week’s YOUR QUESTIONS ANSWERED episode and I’ll see you again in another update next week!
Make sure you also check out our “blog” section for more tips and strategies or send me an email to [email protected] with your questions!
Or you can call us! Find phone numbers on our contact tab.
Also check out our Ebook section where you get more Ebooks, Videos and Audio recordings and where you can also get 1:1 counselling/consulting with me via Skype, over the phone or via email by clicking on the products tab!
This is Patrik Hutzel from INTENSIVECAREHOTLINE.COM and I’ll see you again next week with another update!
Related Articles:
Related Articles:
 MY AUNTY IS IN INTENSIVE CARE ON ECMO FOR ARDS, WE’RE VERY WORRIED SHE MAY DIE! HELP! (PART 9)
MY HUSBAND OF 24 YEARS WAS IN ICU AFTER CARDIAC ARREST AND HE DIED! IT WAS HORRIBLE AND I THINK HE COULD HAVE BEEN SAVED WITH A MORE POSITIVE INTENSIVE CARE TEAM!
My 40 year old brother has been in ICU for 4 weeks after bowel obstruction and Sepsis! He’s still ventilated with tracheostomy and I don’t want him to die, help!
My 84 year old Dad has been in ICU for three months! He’s ventilated with a tracheostomy, the doctors want to let him die and turn off the ventilator! We want to take him home instead, what are our options? (PART 1)
My 84 year old Dad has been in ICU for three months! He’s ventilated with a tracheostomy, the doctors want to let him die and turn off the ventilator! We want to take him home instead, what are our options? (PART 4)
MY AUNTY IS IN INTENSIVE CARE ON ECMO FOR ARDS, WE’RE VERY WORRIED SHE MAY DIE! HELP! (PART 9)
MY HUSBAND OF 24 YEARS WAS IN ICU AFTER CARDIAC ARREST AND HE DIED! IT WAS HORRIBLE AND I THINK HE COULD HAVE BEEN SAVED WITH A MORE POSITIVE INTENSIVE CARE TEAM!
My 40 year old brother has been in ICU for 4 weeks after bowel obstruction and Sepsis! He’s still ventilated with tracheostomy and I don’t want him to die, help!
My 84 year old Dad has been in ICU for three months! He’s ventilated with a tracheostomy, the doctors want to let him die and turn off the ventilator! We want to take him home instead, what are our options? (PART 1)
My 84 year old Dad has been in ICU for three months! He’s ventilated with a tracheostomy, the doctors want to let him die and turn off the ventilator! We want to take him home instead, what are our options? (PART 4)