


What is Cardiomyopathy?
Cardiomyopathy (literally “heart muscle disease”) is the measurable deterioration of the function of the myocardium(the heart muscle) for any reason, usually leading to Heart Failure. Common symptoms are breathlessness and peripheral edema (swelling of the legs). People with cardiomyopathy are often at risk of dangerous forms of irregular heart beat and sudden cardiac death.The most common form of cardiomyopathy is dilated cardiomyopathy. Cardiomyopathy is not the result of pericardial, hypertensive, congenital or ischaemic disease.
- What does the cardiovascular system do?
- Poor or abnormal function of the cardiovascular system
- Different types of Cardiomyopathy
- What Happens in Intensive Care/Coronary Care?
- Signs& Symptoms
- Tests
- Treatment options
- How long will your loved one remain in Intensive Care?
What does the cardiovascular system do?
The essential components of the human cardiovascular system are the heart, lungs, blood, and blood vessels. It includes: the pulmonary circulation, a “loop” through the lungs where blood is oxygenated and the systemic circulation, a “loop” through the rest of the body to provide oxygenated blood. An average adult contains five to six quarts (roughly 4.7 to 5.7 liters) of blood, accounting for approximately 7% of their total body weight. Blood consists of plasma, red blood cells, white blood cells, and platelets. Also, the digestive system works with the circulatory system to provide the nutrients the system needs to keep the heart pumping.
The heart is at the centre, basically distributing blood from the ‘central pump’ with the blood vessels the pipes of the body, trying to reach every corner of the body. The cardiovascular system also passes nutrients (such as amino acids, electrolytes and lymph), gases(Oxygen and Carbon Dioxide), hormones, blood cells, etc. to and from cells in the body to help fight diseases, stabilize body temperature and pH, and to maintain blood pressure.
In the heart there is one atrium and one ventricle for each circulation, and with both a systemic and a pulmonary circulation there are four chambers in total: left atrium, left ventricle, right atrium and right ventricle. The right atrium is the upper chamber of the right side of the heart. The blood that is returned to the right atrium is de-oxygenated (poor in oxygen) and passed into the right ventricle to be pumped through the pulmonary artery to the lungs for re-oxygenation(inhalation) and removal of carbon dioxide(exhalation). The left atrium receives newly oxygenated blood from the lungs as well as the pulmonary vein which is passed into the strong left ventricle to be pumped through the aorta to the different organs of the body.The left side of the heart then receives oxygen rich blood from the lungs and pumps this blood into the Aorta and arteries of the body. This pumping action is a complex well-coordinated activity that cannot be fully explained here. The heart itself, receives oxygenated blood supply via the left and right coronary arteries.
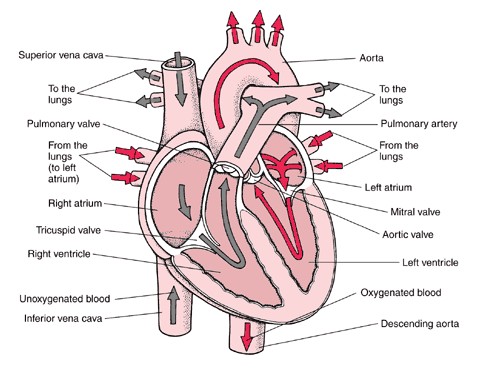
This image was sourced using a google image search
Poor or abnormal function of the cardiovascular system
May be a result of:
- Insufficient blood supply due to dehydration, bleeding or swelling;
- A poor blood supply to the heart, where there is not enough oxygen and other nutrients for its work;
- Poor lung function or obstruction to blood flow in the lungs, which places a strain on the heart muscle;
- Too many or too few electrolytes (eg. potassium, magnesium) that cause irregular heartbeats or dangerous rhythms in the heart.
- Weakness of blood vessel walls.
- Heart muscle weakness
- unhealthy lifestyle such as alcohol consumption, smoking, obesity
Different types of Cardiomyopathy
Dilated cardiomyopathy- DCM is a condition in which the heart becomes weakened and enlarged and cannot pump blood efficiently. The decreased heart function can affect the lungs, liver, and other body systems.
DCM is one of the cardiomyopathies, a group of diseases that primarily affect the myocardium (the muscle of the heart). In DCM a portion of the myocardium is dilated, often without any obvious cause. Left or right ventricular systolic pump function of the heart is impaired, leading to progressive cardiac enlargement and hypertrophy, a process called remodeling.
Dilated cardiomyopathy is the most common form of non-ischemic cardiomyopathy. It occurs more frequently in men than in women, and is most common between the ages of 20 and 60 years. About one in three cases of congestive heart failure (CHF) is due to dilated cardiomyopathy.
Hypertrophic cardiomyopathy (HCM) is a primary disease of the myocardium (the muscle of the heart) in which a portion of the myocardium is hypertrophied (thickened) without any obvious cause. The occurrence of hypertrophic cardiomyopathy is a significant cause of sudden unexpected cardiac death in any age group and as a cause of disabling cardiac symptoms. Younger people are likely to have a more severe form of hypertrophic cardiomyopathy. With HCM, the sarcomeres (contractile elements) in the heart increase in size, which results in the thickening of the heart muscle. In addition, the normal alignment of muscle cells is disrupted, a phenomenon known as myocardial disarray. HCM also causes disruptions of the electrical functions of the heart. HCM is most commonly due to a mutation in one of 9 sarcomeric genes that results in a mutated protein in the sarcomere, the primary component of the myocyte (the muscle cell of the heart).
Restrictive cardiomyopathy(RCM) (a.k.a. Obliterative cardiomyopathy, once known as “constrictive cardiomyopathy”) is a form of cardiomyopathy in which the walls are rigid, and the heart is restricted from stretching and filling with blood properly.
It is the least common of the three original subtypes of cardiomyopathy, which includes hypertrophic and dilated as well as restrictive. It should not be confused with constrictive pericarditis, a disease which presents similarly but is very different in treatment and prognosis.
Rhythm and contractility of the heart may be normal, but the stiff walls of the heart chambers (atria and ventricles) keep them from adequately filling, reducing preload and end-diastolic volume.
Thus, blood flow is reduced, and blood volume that would normally enter the heart is backed up in the circulatory system. In time, restrictive cardiomyopathy Patients develop diastolic dysfunction and eventually heart failure.
Untreated hearts with RCM often develop the following characteristics: Biatrial enlargement, thickened LV walls (with normal chamber size), thickened RV free wall (with normal chamber size), elevated right atrial pressure (>12mmHg), moderate pulmonary hypertension, normal systolic function, poor diastolic function, typically Grade III – IV Diastolic heart failure.
Arrhythmogenic right ventricular cardiomyopathy(ARVD) ARVD is caused by genetic defects of the parts of heart muscle (also called myocardium or cardiac muscle) known as desmosomes, areas on the surface of heart muscle cells which link the cells together. The desmosomes are composed of several proteins, and many of those proteins can have harmful mutations.
The disease is a type of non- ischaemic cardiomyopathy that involves primarily the right ventricle. It is characterized by hypo-kinetic areas involving the free wall of the right ventricle, with fibrofatty replacement of the right ventricular myocardium, with associated arrhythmia’s originating in the right ventricle.
The image above was found at this Website
What happens in Intensive Care/ Coronary Care?
When a person is admitted with a diagnosis of cardiomyopathy the main aims of therapy are to rest the person, to reduce the workload of the heart and to improve the pumping ability of the heart. This treatment is generally drug therapy with drugs such as Dobutamine, Milrinone or Levosimendan, which aids in improving the pumping action of the heart muscle and treatment to ensure the proper volume of blood in the body. Patients may be admitted to either an Intensive care Unit or a Coronary Care Unit depending on the situation and also depending on the capabilities(acuity, skills and equipment) of the unit.
Signs and Symptoms
Symptoms and signs may mimic those of almost any form of heart disease. Chest pain is common. Mild myocarditis or cardiomyopathy is frequently asymptomatic; severe cases are associated with heart failure, arrhythmia’s, and systemic embolization. Manifestations of the underlying disease (e.g., Chagas’ disease) may be prominent. Most Patients with biopsy-proven myocarditis report a recent viral prodrome preceding cardiovascular symptoms.
ECG abnormalities are often present, although the changes are frequently nonspecific. A pattern characteristic of left ventricular hypertrophy may be present. Flat or inverted T waves are most common, often with low-voltage QRS complexes. Intraventricular conduction defects and bundle branch block, especially left bundle branch block, are also common. An echocardiogram is useful to detect wall motion abnormalities or a pericardial effusion. Chest radiographs can be normal or can show evidence of congestive heart failure with pulmonary edema or cardiomegaly. Other signs& symptoms include
- Shortness of breath(especially when laying down) due to collection of fluid in the lungs
- Palpitations – the sensation of feeling the heart beat
- Dizziness
- Cough
- Loss of appetite
- Increased fatigue and decreased exercise tolerance due to the heart’s inability to increase its workload with increased demand
- Increased weight and swelling of hands, legs or feet due to fluid retention
- Low blood pressure due to failure of the cardiovascular system to compensate for the failing heart
Tests that may be done in the Intensive Care Unit
- Physical Examination
- Chest X-ray
- Blood tests(Blood& Pathology tests in Intensive Care)
- Ultrasound of the heart
- Electrocadiograph(ECG)
- Urine tests
Treatment options
Treatment depends on the type and the severity of cardiomyopathy and condition of disease, but may include medication (conservative treatment) or iatrogenic/implanted pacemakers for slow heart rates, defibrillators for those prone to fatal heart rhythms, Ventricular Assist Devices(LVADs) or ECMO(Extracorporeal Membrane Oxygenation) for severe heart failure, or ablation for recurring dysrhythmias that cannot be eliminated by medication or cardioversion. The goal of treatment is often symptom relief, and some patients may eventually require a heart transplant. Treatment of cardiomyopathy (and other heart diseases) using alternative methods such as stem cell therapy is commercially available but is not supported by convincing evidence.
Patients with mild to moderate symptoms will generally be managed by the cardiac team in a coronary care unit (or combined ICU/CCU). However some Patients may present with severe symptoms and may require the full support of an ICU.
- Initially oxygen and respiratory support might be commenced via na oxygen mask or via Non- Invasive Ventilation(NIV) or BIPAP ventilation
- Full ventilation using a Ventilators(Breathing Machine) and a Breathing Tube (endotracheal tube) may be required to improve and maintain the oxygen delivery
- Sedation may be used if your loved one is in an induced coma
- Your loved one will require monitoring using a Bedside Monitors and an Arterial Catheter(Arterial Line)
- You can expect your loved one to have frequent Chest X-rays and blood tests(Blood& Pathology tests in Intensive Care) especially arterial blood gases (ABGs)
- Infusion pumps are administering drugs to support your loved ones blood pressure and haemodynamic system, as well as intravenous fluids may be administered via a central venous catheter/ CVC(Central Venous Lines)
- Use of a Pulmonary Artery Catheters or a PICCO catheter to closely monitor cardiac function is not uncommon.
- An NG Tube (Nasogastric Tubes) is usually inserted into your loved ones stomach, in order to commence nutrition or to remove fluids
- Urine Output is usually measured hourly, after insertion of a Urinary Catheter
Drug Treatments
A variety of drug therapies are used to treat heart failure:
- ACE inhibitors – this group of drugs deceases the workload of the heart by lowering blood pressure and preventing fluid retention by the kidneys;
- Diuretics – increase urine production to treat the fluid retention
- Vasodilators – dilate blood vessels which decrease the workload of the heart;
- Beta blocking agents – slow the heart rate and this decreases the workload of the heart;
- Antiarrhythmic drugs – keep the heart in a normal heart rhythm;
- Inotropic drugs -strengthen heart contraction i.e. Dobutamine, Milrinone, Levosimendan
How long will your loved one remain in Intensive Care?
The time that the person will remain in Intensive Care or Coronary Care will vary depending on the prognosis of your loved one . The prognosis of Patients with heart failure depends primarily on the nature of the underlying heart disease and if the precipitating factor bringing the person into hospital can be treated effectively. Some Patients with severe heart failure may require to be put on a waiting list for a heart transplant. If your loved one is on a waiting list for heart transplant and if your loved ones heart is very weak an LVAD(Ventricular Assist Devices) or ECMO(Extracorporeal Membrane Oxygenation) may be bridging therapies/devices until a heart becomes available.
The team of specialist doctors and Nurses working in the Intensive Care Unit will be able to help give you information on each specific case.
Internet Links
- http://www.heart.org/HEARTORG/ USA heart foundation
- NSW health Internet
- Heart Health and Cardiac Rehabilitation (includes translation to Arabic, Greek, Italian, Russian and Spanish)
- National Heart Foundation – Australia
- Living well with chronic heart failure – translations (scroll to bottom of page)
- National Heart Foundation – New Zealand
- British Heart Foundation
- Heart Beat Victoria
Any Questions?
Of course, if you have any questions or concerns, please discuss them with the ICU nurses and doctors.
All Intensive Care interventions and procedures carry a degree of potential risk even when performed by skilled and experienced staff. Please discuss these issues with the medical and nursing staff who are caring for your loved one.
The information contained in this sheet is general in nature and therefore cannot reflect individual patient variation. It is meant as a back up to specific information which will be discussed with you by the Doctors and Nurses caring for your loved one. INTENSIVE CARE HOTLINE attests to the accuracy of the information contained here BUT takes no responsibility for how it may apply to an individual Patient. Please refer to the Disclaimer.
Related articles:
- How long does a cardiac arrest patient stay in Intensive Care?
- Six weeks in Intensive Care after Cardiac Surgery and my mother isn’t getting any better…
- How long can a breathing tube or an endotracheal tube can stay in?
- How long should a Patient be on a ventilator before having a Tracheostomy?
- How long is a Patient kept on a BIPAP machine in Intensive Care?
- What is an induced coma and why is my critically ill loved one in an induced coma?
- The 3 most dangerous mistakes that you are making but you are unaware of, if your loved one is a critically ill Patient in Intensive Care
- How to always achieve your goals whilst your loved one is critically ill in Intensive Care
- Why you must make up your own mind about your critically ill loved one’s situation in Intensive Care even if you’re not a doctor or a nurse!
- Follow this proven 5 step process on how to be in control and influential if your loved one is a long-term Patient in Intensive Care
- How to quickly take control and have real power and influence if your loved one is critically ill in Intensive Care
- Why does my loved one need a Tracheostomy in Intensive Care?
- Tracheostomy and weaning off the ventilator in Intensive Care, how long can it take?
- My sister has been in ICU for 21 weeks with Tracheostomy and still ventilated. What do we need to do?
- Severe lung failure and my aunty is not expected to survive…
- Be more selfish if your loved one is critically ill in Intensive Care
- 3 quick steps on how to position and prepare yourself well mentally, whilst your loved one is critically ill in Intensive Care
- How to get what you want whilst your loved one is critically ill in Intensive Care
- 5 steps to become a better negotiator if your loved one is critically ill in Intensive Care
- 5 Ways to have control, power and influence while your loved one is critically ill in Intensive Care
- How to make sure that your values and beliefs are known whilst your loved one is critically ill in Intensive Care
- How to make sure that “what you see is always what you get” whilst your loved one is critically ill in Intensive Care
- What the doctors and the nurses behaviour in Intensive Care is telling you about the culture in a unit
- How long does it take to wake up from a Traumatic brain injury or severe head injury
- How to take control if your loved one has a severe brain injury and is critically ill in Intensive Care
- Family Meetings in Intensive Care or the Elephant in the Room
- What you need to do if your loved one is dying in Intensive Care(part one)
- What you need to do if your loved one is dying in Intensive Care(part two)
- Intensive Care at its best?
- How INTENSIVECAREHOTLINE.COM Can Help You
- What you and your Family need to do if your critically ill loved one is very sick in Intensive Care and faces an uncertain future
- How long can somebody stay in Intensive Care?
- My Family can’t agree on what’s best for my sister in Intensive Care…Help!
- My husband is dying in Intensive Care, but we need more time…
- My mother sustained serious brain damage after a stroke and she now is in multi- organ failure