


What is Diabetic Coma?
Diabetic coma is a reversible form of coma found in people with diabetes mellitus. It is a medical emergency.
Three different types of diabetic coma are identified:
- Severe diabetic hypoglycemia
- Diabetic ketoacidosis advanced enough to result in unconsciousness from a combination of severe hyperglycemia, dehydration and shock, and exhaustion
- Hyperosmolar nonketotic coma in which extreme hyperglycemia and dehydration alone are sufficient to cause unconsciousness.
In most medical contexts, the term diabetic coma refers to the diagnostical dilemma posed when a physician is confronted with an unconscious Patient about whom nothing is known except that he has diabetes. An example might be a physician working in an emergency department who receives an unconscious Patient wearing a medical identification tag saying DIABETIC. Paramedics may be called to rescue an unconscious person by friends who identify him as diabetic. Brief descriptions of the three major conditions are followed by a discussion of the diagnostic process used to distinguish among them, as well as a few other conditions which must be considered.
An estimated 2 to 15 percent of diabetics will suffer from at least one episode of diabetic coma in their lifetimes as a result of severe hypoglycemia.
- What is diabetes?
- Diabetic Ketoacidosis (DKA)
- Hyperosmolar Hypoglycemic Non-Ketotic Coma (HHNKC)
- Hypoglycemic Coma
- What happens In Intensive Care?
- How long will your loved one remain in Intensive Care?
- Internet Links
What is Diabetes?
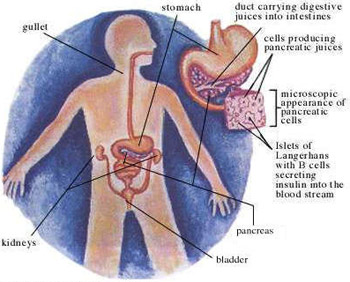
Diabetes mellitus, or simply diabetes, is a group of metabolic diseases in which a person has high blood sugar, either because the pancreas does not produce enough insulin, or because cells do not respond to the insulin that is produced.This high blood sugar produces the classical symptoms of polyuria (frequent urination), polydipsia (increased thirst) and polyphagia (increased hunger).
There are three main types of diabetes mellitus (DM).
- Type 1 DM results from the body’s failure to produce insulin, and presently requires the person to inject insulin or wear an insulin pump. This form was previously referred to as “insulin-dependent diabetes mellitus” (IDDM) or “juvenile diabetes”.
- Type 2 DM results from insulin resistance, a condition in which cells fail to use insulin properly, sometimes combined with an absolute insulin deficiency. This form was previously referred to as non insulin-dependent diabetes mellitus (NIDDM) or “adult-onset diabetes”.
- The third main form, gestational diabetes occurs when pregnant women without a previous diagnosis of diabetes develop a high blood glucose level. It may precede development of type 2 DM.
All forms of diabetes have been treatable since insulin became available in 1921, and type 2 diabetes may be controlled with medications. Insulin and some oral medications can cause hypoglycemia (low blood sugars), which can be dangerous if severe. Both types 1 and 2 are chronic conditions that cannot be cured. Pancreas transplants have been tried with limited success in type 1 DM; gastric bypass surgery has been successful in many with morbid obesity and type 2 DM. Gestational diabetes usually resolves after delivery.
Diabetic Keto-acidosis (DKA)
Diabetic ketoacidosis (DKA) is a potentially life-threatening complication in patients with diabetes mellitus. It happens predominantly in those with type 1 diabetes, but it can occur in those with type 2 diabetes under certain circumstances. DKA results from a shortage of insulin; in response the body switches to burning fatty acids and producing acidic ketone bodies that cause most of the symptoms and complications.
DKA may be the first symptom of previously undiagnosed diabetes, but it may also occur in people known to have diabetes as a result of a variety of causes, such as inter-current illness or poor compliance with insulin therapy. Thirst, Vomiting, frequent urination, dehydration, deep gasping breathing, confusion and occasionally coma are typical symptoms. DKA is diagnosed with blood and urine tests; it is distinguished from other, rarer forms of ketoacidosis by the presence of high blood sugar levels. Treatment involves intravenous fluids to correct dehydration, insulin to suppress the production of ketone bodies, treatment for any underlying causes such as infections, and close observation to prevent and identify complications.
DKA is a medical emergency, and without treatment it can lead to death. DKA was first described in 1886; until the introduction of insulin therapy in the 1920s it was almost universally fatal. It now carries a mortality of less than 1% with adequate and timely treatment.
Hyperosmolar Hyperglycemic Non-Ketotic Coma (HHNKC)
Hyperglycemic hyperosmolar nonketotic coma (HHNKC) is an extremely serious complication of type 2 diabetes, most often occurring in those who are non-insulin dependent. This diabetic emergency is similar to diabetic ketoacidosis (DKA) however there are some notable differences.
HHNKC is caused by severely elevated blood glucose levels, usually over 600 mg/dl(BSL usually higher than in DKA). Symptoms can include weakness, increased thirst, dehydration, frequent urination, nausea, lethargy, confusion and ultimately, convulsions, and coma. Onset of these symptoms can be slow and insidious, building over a period of days or weeks.
HHNKC frequently happens in the elderly and is usually precipitated by another illness, such as infection or flu, or sometimes a chronic condition such as congestive heart failure or renal failure. HHNKC is an emergency that requires immediate medical care.
HHNKC is treated the same as DKA. Patients will require insulin and large amounts of fluids.
Hypoglycemic Coma
Hypoglycemic Coma(not to be confused with hyperglycemia) is an abnormally diminished content of glucose in the blood.The term literally means “low sugar blood”. It can produce a variety of symptoms and effects but the principal problems arise from an inadequate supply of glucose to the brain, resulting in impairment of function (neuroglycopenia). Effects can range from mild dysphoria to more serious issues such as seizures, unconsciousness, and (rarely) permanent brain damage or death.
A Patient will become unconscious very quickly and requires a source of glucose urgently. All diabetics should have a emergency plan in place in the event of this occurring. This would usually include keeping a source of rapid glucose on hand in case symptoms occur. Treatment of hypoglycemic coma is usually a dose of concentrated glucose and most Patients will recover within minutes. Admission to an intensive care unit would not be required unless there are other problems.
The most common forms of hypoglycemia occur as a complication of treatment of diabetes mellitus with insulin or oral medications. Hypoglycemia is less common in non-diabetic persons, but can occur at any age. Among the causes are excessive insulin produced in the body (hyperinsulinemia), inborn error of metabolism, medications and poisons, alcohol, hormone deficiencies, prolonged starvation, alterations of metabolism associated with infection, and organ failure.
Hypoglycemia is treated by restoring the blood glucose level to normal by the ingestion or administration of dextrose or carbohydrate foods. In more severe circumstances it is treated by injection or infusion of glucagon. Recurrent hypoglycemia may be prevented by reversing or removing the underlying cause, by increasing the frequency of meals, with medications like diazoxide, octreotide, or glucocorticoids, or by surgical removal of much of the pancreas(pancreatectomy).
The level of blood glucose low enough to define hypoglycemia may be different for different people, in different circumstances, and for different purposes, and occasionally has been a matter of controversy. Most healthy adults maintain fasting glucose levels above 4.0 mmol/L (72 mg/dl), and develop symptoms of hypoglycemia when the glucose falls below 4 mmol/L
What happens In Intensive Care?
- If your loved one is suffering from DKA or HHNKC he or she will require insulin and rapid rehydration (fluid replacement) with intravenous fluid.
- Admission to a high dependency area is likely, as they will need frequent blood tests , especially arterial blood gases and a larger amount of intravenous fluids. An insulin infusion will be required to ensure a reliable source of insulin and the blood sugar level (BSL) will be checked frequently. This will be done hourly to start, then less often as the BSL stabilises and falls.
- An Arterial Catheter may be inserted(Arterial line insertion) for frequent blood tests such as Blood sugar levels(BSL) and Electrolyte checks such as potassium and Magnesium, osmolality (blood concentration) and acid-base status
- Once the BSL has been controlled a glucose infusion will probably be started to prevent the BSL from falling too quickly
- Your loved one will be connected to a Patient monitor(Bedside Monitors)
- An indwelling urinary catheter will be used to accurately monitor hourly urine output and the amount of ketones in the urine. The amount of ketones is a good indicator of whether the DKA is resolving and your loved ones condition improving
- Generally your loved one will be ‘nil by mouth’ until the urine is ketone free
- Occasionally a Nasogastric Tubes (NG Tube) may be needed if your loved one is vomiting a lot. Replacement of the body’s electrolytes, especially potassium will also be required
How long will your loved one remain in Intensive Care?
Your loved ones stay in Intensive Care will usually only be a few days unless they have other problems or complications.
Internet Links
- Diabetes Australia
- NSWHealth – Multicultural Communication Pages, Diabetes Link Page
- American Diabetes organisation http://www.diabetes.org/
- UK Diabetes organisation http://www.diabetes.org.uk/
Any Questions?
Of course, if you have any questions or concerns, please discuss them with the ICU nurses and doctors.
All Intensive Care interventions and procedures carry a degree of potential risk even when performed by skilled and experienced staff. Please discuss these issues with the medical and nursing staff who are caring for your loved one.
The information contained on this page is general in nature and therefore cannot reflect individual Patient variation. It is meant as a back up to specific information which will be discussed with you by the Doctors and Nurses caring for your loved one. INTENSIVE CARE HOTLINE attests to the accuracy of the information contained here BUT takes no responsibility for how it may apply to an individual Patient. Please refer to the full disclaimer.
Related Articles:
- How long can a breathing tube or an endotracheal tube can stay in?
- How long should a Patient be on a ventilator before having a Tracheostomy?
- How long is a Patient kept on a BIPAP machine in Intensive Care?
- What is an induced coma and why is my critically ill loved one in an induced coma?
- The 3 most dangerous mistakes that you are making but you are unaware of, if your loved one is a critically ill Patient in Intensive Care
- How to always achieve your goals whilst your loved one is critically ill in Intensive Care
- Why you must make up your own mind about your critically ill loved one’s situation in Intensive Care even if you’re not a doctor or a nurse!
- Follow this proven 5 step process on how to be in control and influential if your loved one is a long-term Patient in Intensive Care
- How to quickly take control and have real power and influence if your loved one is critically ill in Intensive Care
- Why does my loved one need a Tracheostomy in Intensive Care?
- Tracheostomy and weaning off the ventilator in Intensive Care, how long can it take?
- My sister has been in ICU for 21 weeks with Tracheostomy and still ventilated. What do we need to do?
- Severe lung failure and my aunty is not expected to survive…
- Be more selfish if your loved one is critically ill in Intensive Care
- 3 quick steps on how to position and prepare yourself well mentally, whilst your loved one is critically ill in Intensive Care
- How to get what you want whilst your loved one is critically ill in Intensive Care
- 5 steps to become a better negotiator if your loved one is critically ill in Intensive Care
- 5 Ways to have control, power and influence while your loved one is critically ill in Intensive Care
- How to make sure that your values and beliefs are known whilst your loved one is critically ill in Intensive Care
- How to make sure that “what you see is always what you get” whilst your loved one is critically ill in Intensive Care
- What the doctors and the nurses behaviour in Intensive Care is telling you about the culture in a unit
- How long does it take to wake up from a Traumatic brain injury or severe head injury
- How to take control if your loved one has a severe brain injury and is critically ill in Intensive Care
- Family Meetings in Intensive Care or the Elephant in the Room
- What you need to do if your loved one is dying in Intensive Care(part one)
- What you need to do if your loved one is dying in Intensive Care(part two)
- Intensive Care at its best?
- How INTENSIVECAREHOTLINE.COM Can Help You
- What you and your Family need to do if your critically ill loved one is very sick in Intensive Care and faces an uncertain future
- How long can somebody stay in Intensive Care?
- My Family can’t agree on what’s best for my sister in Intensive Care…Help!
- My husband is dying in Intensive Care, but we need more time…
- My mother sustained serious brain damage after a stroke and she now is in multi- organ failure